filmov
tv
Medial Collateral Ligament Injuries - Everything You Need To Know - Dr. Nabil Ebraheim
Показать описание
Dr. Ebraheim’s educational animated video describes the condition medial collateral ligament (MCL) injury.
Follow me on twitter:
Medial Collateral Ligament Injuries
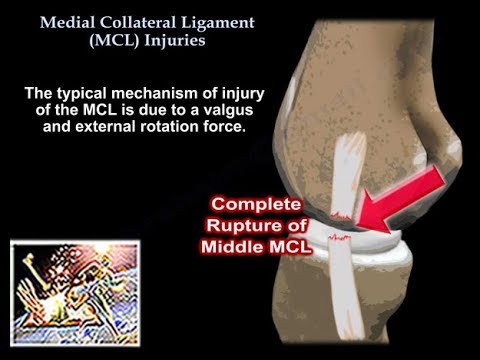
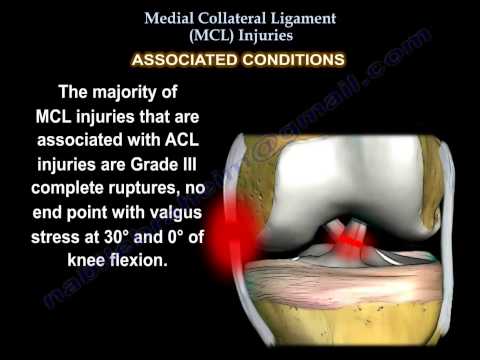
The medial collateral ligament is one of four major ligaments of the knee. The medial collateral ligament extends from the medial epicondyle of the femur to below the medial condyle of the tibia. The MCL is a static stabilizer composed of superficial (primary) and deep (secondary) portions that are restraints to valgus stress. The superficial MCL is the primary restraint to valgus stress. The proximal attachment is located on the posterior aspect of the medial femoral condyle. The distal attachment is located at the metaphyseal region of the tibia, about 5cm distal to the joint, lying beneath the pes anserinus. The Deep MCL assists as a secondary restraint to valgus stress. The Deep MCL inserts directly into the edge of the tibial plateau and meniscus. It may be separated from the superficial layer by a bursa. The joined tendons of the Sartorius, gracilis, and semitendinosus muscles cross on top of the lower part of the MCL. The pes anserine bursa is located anterior to the insertion of the medial collateral ligament into the tibia. The MCL’s primary function is to be a restraint to valgus stress. The MCL is the most commonly injured ligament of the knee. The typical mechanism of injury of the MCL is due to a valgus and external rotation force. A direct blow to the knee usually causes a complete rupture of the MCL. Rupture may occur proximally or distally. Tears of the proximal MCL have a greater healing rate; however, tears of the distal MCL may not heal well (similar to a Stener lesion of the thumb). Injury to the ACL comprise up to 95% of associated injuries. Rupture of the ACL causes anterolateral rotatory instability. The majority of MCL injuries that are associated with ACL injuries are Grade III complete ruptures, no end point with valgus stress at 30° and 0° of knee flexion. Up to 5% of isolated MCL injuries are associated with meniscal tears. Not a common injury. MCL sprains are classified into three different grades. Grade I injuries are a sprain or stretching injury. Grade II injuries consist of a partial tear of the MCL. Grade III tears are a complete tear of the ligament with no end point with valgus stress at 30° of knee flexion.
A medial collateral ligament injury will typically create a “popping” sensation. Pain and tenderness is usually found higher than the joint line. During the physical examination, tenderness will be discovered along the medial aspect of the knee. A positive valgus stress test at 30° of knee flexion indicates injury to the superficial MCL. Opening around 1 cm indicates a Grade III complete tear of the MCL. A positive valgus stress test at 0° of knee extension indicates posteromedial capsule or cruciate ligament injury in addition to MCL injury (combined injury). The physician should always evaluate for other injuries to the ACL, PCL, or medial meniscal tear. Radiographs are usually normal; however, they may show calcification at the medial femoral site (Pellegrini-Stieda Syndrome). Calcification due to chronic MCL deficiency at the medial femoral insertion site. A pediatric patient with a knee injury and a suspected salter fracture should have stress view x-rays performed to rule out a growth plate injury. Growth plates are weaker than ligaments and it may be more beneficial to have an MRI performed rather than stress view x-rays. An MRI is the study of choice as it identifies the location and extent of the MCL injury.
Treatment typically consists of NSAIDs, rest, and therapy. A minor sprain of the MCL will require therapy with a return to play in about a week. A brace may be used if the injury is classified as a Grade II and they will return to play in about 2-4 weeks. With Grade III injuries, there will be a return to play in about 6-8 weeks. Surgery is performed in Grade III injuries with a multiple ligament injury, especially with distal avulsion fractures. If there is chronic instability with opening in full extension, a reconstruction should be performed. An additional arthroscopy may be needed to rule out associated injuries. In combined MCL and ACL injuries, usually surgery for the ACL is delayed until the MCL heals (up to eight weeks) and then an ACL brace should be used. Complications consist of stiffness and loss of motion. Laxity is associated with distal MCL injuries. Functional bracing may reduce an MCL injury in football players, particularly with interior linemen.
Follow me on twitter:
Medial Collateral Ligament Injuries
The medial collateral ligament is one of four major ligaments of the knee. The medial collateral ligament extends from the medial epicondyle of the femur to below the medial condyle of the tibia. The MCL is a static stabilizer composed of superficial (primary) and deep (secondary) portions that are restraints to valgus stress. The superficial MCL is the primary restraint to valgus stress. The proximal attachment is located on the posterior aspect of the medial femoral condyle. The distal attachment is located at the metaphyseal region of the tibia, about 5cm distal to the joint, lying beneath the pes anserinus. The Deep MCL assists as a secondary restraint to valgus stress. The Deep MCL inserts directly into the edge of the tibial plateau and meniscus. It may be separated from the superficial layer by a bursa. The joined tendons of the Sartorius, gracilis, and semitendinosus muscles cross on top of the lower part of the MCL. The pes anserine bursa is located anterior to the insertion of the medial collateral ligament into the tibia. The MCL’s primary function is to be a restraint to valgus stress. The MCL is the most commonly injured ligament of the knee. The typical mechanism of injury of the MCL is due to a valgus and external rotation force. A direct blow to the knee usually causes a complete rupture of the MCL. Rupture may occur proximally or distally. Tears of the proximal MCL have a greater healing rate; however, tears of the distal MCL may not heal well (similar to a Stener lesion of the thumb). Injury to the ACL comprise up to 95% of associated injuries. Rupture of the ACL causes anterolateral rotatory instability. The majority of MCL injuries that are associated with ACL injuries are Grade III complete ruptures, no end point with valgus stress at 30° and 0° of knee flexion. Up to 5% of isolated MCL injuries are associated with meniscal tears. Not a common injury. MCL sprains are classified into three different grades. Grade I injuries are a sprain or stretching injury. Grade II injuries consist of a partial tear of the MCL. Grade III tears are a complete tear of the ligament with no end point with valgus stress at 30° of knee flexion.
A medial collateral ligament injury will typically create a “popping” sensation. Pain and tenderness is usually found higher than the joint line. During the physical examination, tenderness will be discovered along the medial aspect of the knee. A positive valgus stress test at 30° of knee flexion indicates injury to the superficial MCL. Opening around 1 cm indicates a Grade III complete tear of the MCL. A positive valgus stress test at 0° of knee extension indicates posteromedial capsule or cruciate ligament injury in addition to MCL injury (combined injury). The physician should always evaluate for other injuries to the ACL, PCL, or medial meniscal tear. Radiographs are usually normal; however, they may show calcification at the medial femoral site (Pellegrini-Stieda Syndrome). Calcification due to chronic MCL deficiency at the medial femoral insertion site. A pediatric patient with a knee injury and a suspected salter fracture should have stress view x-rays performed to rule out a growth plate injury. Growth plates are weaker than ligaments and it may be more beneficial to have an MRI performed rather than stress view x-rays. An MRI is the study of choice as it identifies the location and extent of the MCL injury.
Treatment typically consists of NSAIDs, rest, and therapy. A minor sprain of the MCL will require therapy with a return to play in about a week. A brace may be used if the injury is classified as a Grade II and they will return to play in about 2-4 weeks. With Grade III injuries, there will be a return to play in about 6-8 weeks. Surgery is performed in Grade III injuries with a multiple ligament injury, especially with distal avulsion fractures. If there is chronic instability with opening in full extension, a reconstruction should be performed. An additional arthroscopy may be needed to rule out associated injuries. In combined MCL and ACL injuries, usually surgery for the ACL is delayed until the MCL heals (up to eight weeks) and then an ACL brace should be used. Complications consist of stiffness and loss of motion. Laxity is associated with distal MCL injuries. Functional bracing may reduce an MCL injury in football players, particularly with interior linemen.
Medial Collateral Ligament Injuries - Everything You Need To Know - Dr. Nabil Ebraheim
 0:02:13
0:02:13
How to diagnose a Medial Collateral Ligament injury
 0:00:47
0:00:47
ACL (Anterior Cruciate Ligament) MCL (Medial Collateral Ligament) Tear and Repair (No Narration)
 0:03:40
0:03:40
Valgus Stress Test of the Knee | Medial Collateral Ligament (MCL) Injury
 0:25:25
0:25:25
MCL Injury Rehab & Exercises (Medial Collateral Ligament Sprain)
 0:01:24
0:01:24
How to test the Medial Collateral ligament (MCL) of the Knee
 0:01:06
0:01:06
ACL and MCL Tear and Surgical Repair - 3D Animation
 0:02:39
0:02:39
Diagnostic Cluster for Medial Collateral Ligament (MCL) Injuries of the Knee
 1:02:07
1:02:07
MSK Review for NPs
 0:01:39
0:01:39
The Visible Athlete: Medial Collateral Ligament (MDL) Injury of the Knee
 0:25:47
0:25:47
MCL Sprains and Tears - Treatment and Exercises
 0:05:34
0:05:34
Medial Collateral Ligament injury , MCL Injuries - Everything You Need To Know - Dr. Nabil Ebraheim
 0:02:23
0:02:23
Understand Knee Ligament Injuries (ACL, PCL, MCL, LCL) - 3D animation
 0:04:09
0:04:09
How long does it take an MCL injury of the knee to heal?
 0:02:01
0:02:01
Symptoms of a MCL Injury
 0:13:03
0:13:03
Top 7 MCL Sprain Treatments - Ask Doctor Jo
 0:02:16
0:02:16
Exercises for Medial Knee Ligament Injury - Overview
 0:02:02
0:02:02
InternalBrace™ MCL Augmentation Repair
 0:04:26
0:04:26
Can I walk with an MCL injury?
 0:00:18
0:00:18
MCL (medial collateral ligament) injury rehab
 0:00:55
0:00:55
MCL Sprain Rehab #shorts
 0:00:16
0:00:16
Find out if your tore your MCL (self test) #shorts
 0:07:28
0:07:28
MCL Tear - 4 Exercises to Rehab Your Knee
 0:08:46
0:08:46
How To Tell If You Have An MCL Injury In Your Knee
Комментарии