filmov
tv
Case Study 25: Right Lower Quadrant Abdominal Pain - CRASH! Medical Review Series

Показать описание
(Disclaimer: The medical information contained herein is intended for physician medical licensing exam review purposes only, and are not intended for diagnosis of any illness. If you think you may be suffering from any medical condition, you should consult your physician or seek immediate medical attention.)
 0:10:17
0:10:17
Case Study 25: Right Lower Quadrant Abdominal Pain - CRASH! Medical Review Series
 0:06:20
0:06:20
How Long To Get From 25% to 15% Body Fat? (Reality Check)
 0:00:27
0:00:27
What to Do if You Didn’t Study
 0:00:53
0:00:53
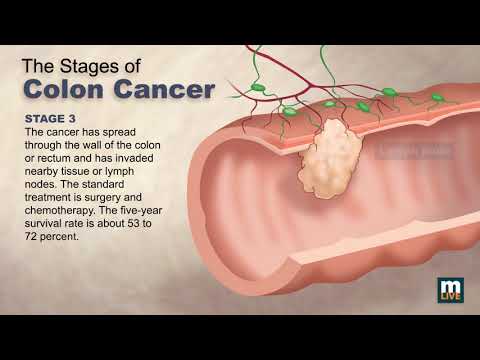
Stages of Colon Cancer
 0:06:49
0:06:49
PART 1 Lower back Pain Case Study
 0:06:14
0:06:14
Patient case study: Is that lower respiratory tract infection viral or bacterial?
 0:05:05
0:05:05
Cerebellum Examination (Stanford Medicine 25)
 0:02:00
0:02:00
2-Minute Neuroscience: Bell's Palsy
 0:01:43
0:01:43
What happens when autistic kids become adults?
 0:02:44
0:02:44
How Traumatic Brain Injury (TBI) Affects Brain Cells - New Research Could Lead to New Treatments
 0:37:04
0:37:04
Case Study #2: Ischemic Stroke
 0:00:37
0:00:37
Coronary artery anatomy - Coronary angiogram
 0:03:35
0:03:35
Autism Spectrum Disorder: 10 things you should know
 0:01:19
0:01:19
How do beta blockers work?
 0:01:03
0:01:03
3D Medical Animation - Congestive Heart Failure
 0:06:37
0:06:37
Sample size Calculation
 0:16:22
0:16:22
Making $150k A Year And Still Feel Broke (CASE STUDY)
 0:09:14
0:09:14
Recipe to losing weight | Anna Verhulst | TEDxMaastricht
 0:00:31
0:00:31
In text citations in Word 2019
 0:02:52
0:02:52
Utm thesis format (margin)
 0:10:01
0:10:01
Congestive Heart Failure Signs & Symptoms (& Why They Occur)
 0:02:25
0:02:25
What Adult ADHD Can Look Like 🔍
 0:00:12
0:00:12
Air hostesses trying to close door 😅 #shorts
 0:00:19
0:00:19
Behind the Scene of the Class after becoming Parents || Work Life Balance ||
Комментарии