filmov
tv
Carpal Tunnel Syndrome - Everything You Need To Know - Dr. Nabil Ebraheim
Показать описание
Dr. Ebraheim’s educational animated video describes describes carpal tunnel syndrome.
Carpal tunnel syndrome is compression of the median nerve at the wrist. It is the most common form of nerve entrapment
What is the carpal tunnel? The carpal tunnel is a narrow passage on the palmar side of the wrist made up of bones and ligaments. The carpal tunnel is narrowest at the level of the hook of hamate.
The carpal tunnel is defined by:
•the scaphoid tubercle and trapezium radially
•hook of hamate and pisiform ulnarly
•Proximal carpal row dorsally (floor)
•Transverse carpal ligament palmarly (roof)
The carpal tunnel consists of:
•Nine flexor tendons,with FPL being the most radial tendon. The FDS for the ring and middle fingers lies volar to the index and small fingers.
The recurrent motor branch of the median nerve has multiple variation of the nerve:
•50% are extraligamentous with recurrent innervation.
•30% are subligamentous with recurrent innervation.
•20% are transligamentous with recurrent innervation.
The median nerve also branches into ulnar and radial divisions.
How does carpal tunnel syndrome occur?
Pressure is placed on the median nerve and other structures by the transverse carpal ligament. The normal resting pressure of a hand in the neutral position without carpal tunnel is 2.5 mmHg. In the wrist without carpal tunnel, flexion or extension of the wrist causes pressure on the median nerve of 30 mmHg. The normal resting pressure of a hand in the neutral position with carpal tunnel is 30 mmHg. In the wrist with carpal tunnel, flexion or extension of the wrist causes pressure on the median nerve of between 90-110 mmHg. When using a splint, the CT pressure increases when the wrist is in extension and is the lowest when the wrist is neutral.
Symptoms of CTS:
•Numbness and tingling in the radial 3 ½ digits. Numbness should be less at the thenar area of the palm.
•Clumsiness and weakness
•Pain and paresthesia that wakes the patient up at night and is relieved by shaking the hand away.
Self-administered hand diagram is the most specific test for carpal tunnel syndrome. Thenar atrophy may be present.
For examination:
•Durkan’s test- carpal tunnel compression test is the most sensitive test to diagnose CTS. It is performed by pressing the thumbs over the carpal tunnel and holding pressure for 30 seconds. The onset of pain or paresthesia in the median nerve distribution within 30 seconds is a positive result.
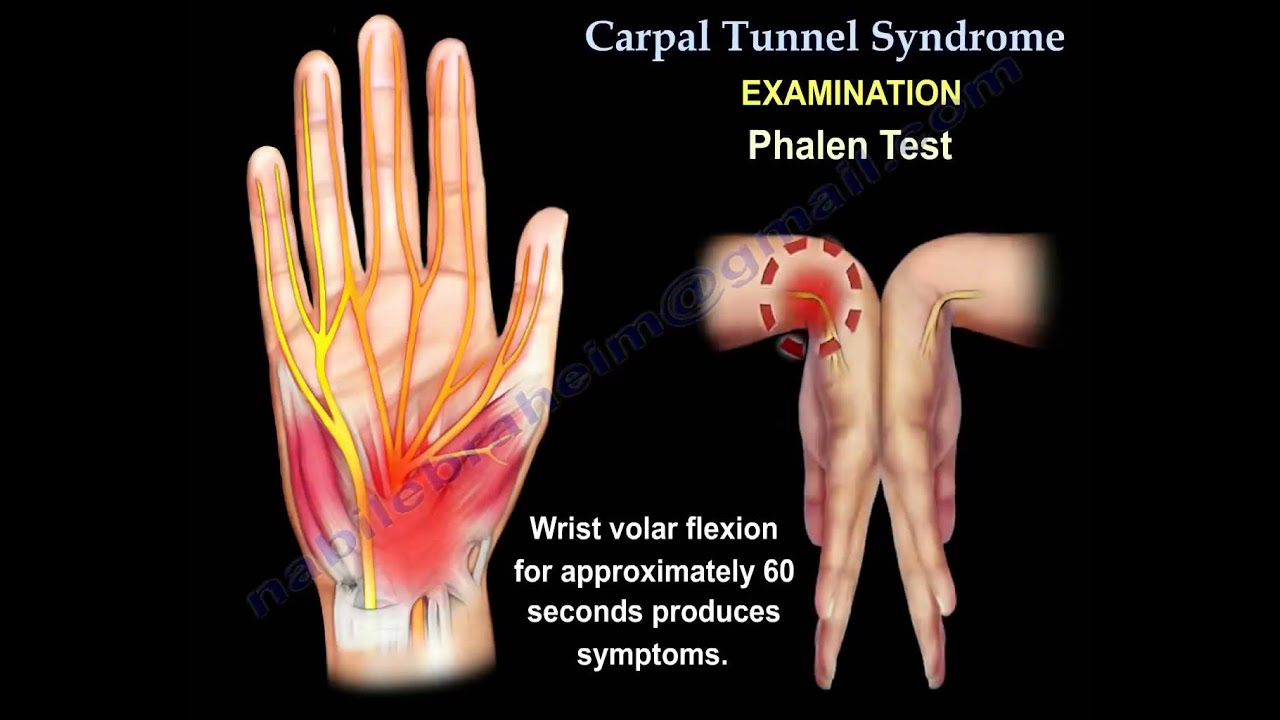
•Phalen test: wrist volar flexion for approximately 60 seconds produces symptoms. Test is performed by tapping on the median nerve over the volar carpal tunnel.
•Semmes-Weinstein testing: most sensitive sensory test for detecting early carpal tunnel syndrome.
•Innervation density test: a- static and moving two point discrimination
Diagnosis of CTS is a clinical diagnosis. Do EMG and nerve conduction studies if surgery is considered. Only subjective evidence of compression neuropathy (routinely used in workmen’s compensation patients). May be negative in about 20% of the patients.
Etiology:
•Repetitive motion and vibration causes thickening of the transverse carpal ligament.
•Pregnancy
•Systemic diseases as diabetes, dialysis, rheumatoid arthritis, obesity, hypothyroidism, amyloidosis and mucopolysaccharidosis.
Risk factors:
•Female •Smoking •Advanced age •Alcoholism •Obesity •Repetitive motion
Comparing surgery with splints, the improvement success rate is 80% with surgery and 54% with splinting at 3 months. 18 months: 90% with surgery and 75% with splint.
Indication for surgery:
•Failure of non-operative management
•Thenar weakness/atrophy
•EMG abnormalities
•Known extrinsic compression from mass lesion.
Open carpal tunnel release results:
•Pillar pain for up to 3-4 months
•Dynamic symptoms resolve rapidly with wrist movement
•Release of the carpal tunnel and duputyren’s contracture at the same time may make the condition worse.
•Static numbness/weakness may take up to a year for improvement plateau.
Outcomes: pinch strength returns in 6 weeks. Grip strength is expected to return to 100% preoperative levels by 12 weeks postoperative. Pinch strength recovers faster than the grip strength. No effect on carpal tunnel release surgery results:
•Internal neurolysis
•Transverse carpal ligament reconstruction
•Tensosynovectomy
•Guyon’s tunnel release.
Causes of carpal tunnel release failure
•Incomplete TCL release
•Incorrect diagnosis
•Double/triple crush
•Peripheral neuropathy
•Space occupying lesion
•Iatrogenic median nerve injury
Become a friend on facebook:
Follow me on twitter:
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
Background music provided as a free download from YouTube Audio Library.
Song Title: Every Step
Carpal tunnel syndrome is compression of the median nerve at the wrist. It is the most common form of nerve entrapment
What is the carpal tunnel? The carpal tunnel is a narrow passage on the palmar side of the wrist made up of bones and ligaments. The carpal tunnel is narrowest at the level of the hook of hamate.
The carpal tunnel is defined by:
•the scaphoid tubercle and trapezium radially
•hook of hamate and pisiform ulnarly
•Proximal carpal row dorsally (floor)
•Transverse carpal ligament palmarly (roof)
The carpal tunnel consists of:
•Nine flexor tendons,with FPL being the most radial tendon. The FDS for the ring and middle fingers lies volar to the index and small fingers.
The recurrent motor branch of the median nerve has multiple variation of the nerve:
•50% are extraligamentous with recurrent innervation.
•30% are subligamentous with recurrent innervation.
•20% are transligamentous with recurrent innervation.
The median nerve also branches into ulnar and radial divisions.
How does carpal tunnel syndrome occur?
Pressure is placed on the median nerve and other structures by the transverse carpal ligament. The normal resting pressure of a hand in the neutral position without carpal tunnel is 2.5 mmHg. In the wrist without carpal tunnel, flexion or extension of the wrist causes pressure on the median nerve of 30 mmHg. The normal resting pressure of a hand in the neutral position with carpal tunnel is 30 mmHg. In the wrist with carpal tunnel, flexion or extension of the wrist causes pressure on the median nerve of between 90-110 mmHg. When using a splint, the CT pressure increases when the wrist is in extension and is the lowest when the wrist is neutral.
Symptoms of CTS:
•Numbness and tingling in the radial 3 ½ digits. Numbness should be less at the thenar area of the palm.
•Clumsiness and weakness
•Pain and paresthesia that wakes the patient up at night and is relieved by shaking the hand away.
Self-administered hand diagram is the most specific test for carpal tunnel syndrome. Thenar atrophy may be present.
For examination:
•Durkan’s test- carpal tunnel compression test is the most sensitive test to diagnose CTS. It is performed by pressing the thumbs over the carpal tunnel and holding pressure for 30 seconds. The onset of pain or paresthesia in the median nerve distribution within 30 seconds is a positive result.
•Phalen test: wrist volar flexion for approximately 60 seconds produces symptoms. Test is performed by tapping on the median nerve over the volar carpal tunnel.
•Semmes-Weinstein testing: most sensitive sensory test for detecting early carpal tunnel syndrome.
•Innervation density test: a- static and moving two point discrimination
Diagnosis of CTS is a clinical diagnosis. Do EMG and nerve conduction studies if surgery is considered. Only subjective evidence of compression neuropathy (routinely used in workmen’s compensation patients). May be negative in about 20% of the patients.
Etiology:
•Repetitive motion and vibration causes thickening of the transverse carpal ligament.
•Pregnancy
•Systemic diseases as diabetes, dialysis, rheumatoid arthritis, obesity, hypothyroidism, amyloidosis and mucopolysaccharidosis.
Risk factors:
•Female •Smoking •Advanced age •Alcoholism •Obesity •Repetitive motion
Comparing surgery with splints, the improvement success rate is 80% with surgery and 54% with splinting at 3 months. 18 months: 90% with surgery and 75% with splint.
Indication for surgery:
•Failure of non-operative management
•Thenar weakness/atrophy
•EMG abnormalities
•Known extrinsic compression from mass lesion.
Open carpal tunnel release results:
•Pillar pain for up to 3-4 months
•Dynamic symptoms resolve rapidly with wrist movement
•Release of the carpal tunnel and duputyren’s contracture at the same time may make the condition worse.
•Static numbness/weakness may take up to a year for improvement plateau.
Outcomes: pinch strength returns in 6 weeks. Grip strength is expected to return to 100% preoperative levels by 12 weeks postoperative. Pinch strength recovers faster than the grip strength. No effect on carpal tunnel release surgery results:
•Internal neurolysis
•Transverse carpal ligament reconstruction
•Tensosynovectomy
•Guyon’s tunnel release.
Causes of carpal tunnel release failure
•Incomplete TCL release
•Incorrect diagnosis
•Double/triple crush
•Peripheral neuropathy
•Space occupying lesion
•Iatrogenic median nerve injury
Become a friend on facebook:
Follow me on twitter:
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
Background music provided as a free download from YouTube Audio Library.
Song Title: Every Step
 0:11:58
0:11:58
Carpal Tunnel Syndrome - Everything You Need To Know [Diagnosis & Natural Treatment]
 0:01:41
0:01:41
Carpal Tunnel Syndrome Explained: Symptoms, Diagnosis, and Treatment Options
 0:12:48
0:12:48
Carpal Tunnel Syndrome - Everything You Need To Know - Dr. Nabil Ebraheim
 0:05:24
0:05:24
Carpal Tunnel Syndrome: Everything You Need to Know
 0:10:30
0:10:30
Carpal Tunnel Syndrome - Causes and Treatments
 0:05:05
0:05:05
How to treat CARPAL TUNNEL SYNDROME at home (and when to get medical advice) | Doctor explains
 0:00:58
0:00:58
Mayo Clinic Minute: What is carpal tunnel syndrome?
 0:07:54
0:07:54
Patient Self Diagnose Carpal Tunnel Syndrome - Everything You Need To Know - Dr. Nabil Ebraheim
 0:09:03
0:09:03
Best Info on CARPAL TUNNEL Syndrome - Everything you need to know about diagnosis & treatment
 0:05:29
0:05:29
Carpal tunnel syndrome - causes, symptoms, diagnosis, treatment & pathology
 0:04:22
0:04:22
Carpal Tunnel Syndrome - Everything You Need to Know
 0:01:44
0:01:44
What Is Carpal Tunnel Syndrome? | UPMC
 0:06:32
0:06:32
Diabetes & Carpal Tunnel Syndrome - Everything You Need To Know - Dr. Nabil Ebraheim
 0:00:50
0:00:50
Relieve Carpal Tunnel Syndrome in Seconds #Shorts
 0:00:58
0:00:58
understanding Carpal Tunnel Syndrome in seconds - Everything You Need To Know - Dr. Nabil Ebraheim
 0:09:25
0:09:25
Carpal Tunnel Syndrome (Diagnosis Explained | Science Based)
 0:08:29
0:08:29
3 BEST Exercises for Carpal Tunnel Syndrome
 0:03:02
0:03:02
Carpal Tunnel Syndrome ,anatomy ,animation - Everything You Need To Know - Dr. Nabil Ebraheim
 0:00:34
0:00:34
Endoscopic Carpal Tunnel Release
 0:10:04
0:10:04
Understanding Carpal Tunnel Syndrome
 0:14:11
0:14:11
Is Carpal Tunnel Syndrome coming from your Neck?
 0:06:16
0:06:16
Carpal Tunnel Syndrome: What You Need to Know
 0:02:34
0:02:34
Carpal Tunnel Syndrome | FAQ with Dr. Sophia Strike
 0:10:50
0:10:50
3 Simple Postural Exercises to Relieve Carpal Tunnel Syndrome
Комментарии