filmov
tv
ABG Interpretation: The Anion Gap (Lesson 5)
Показать описание
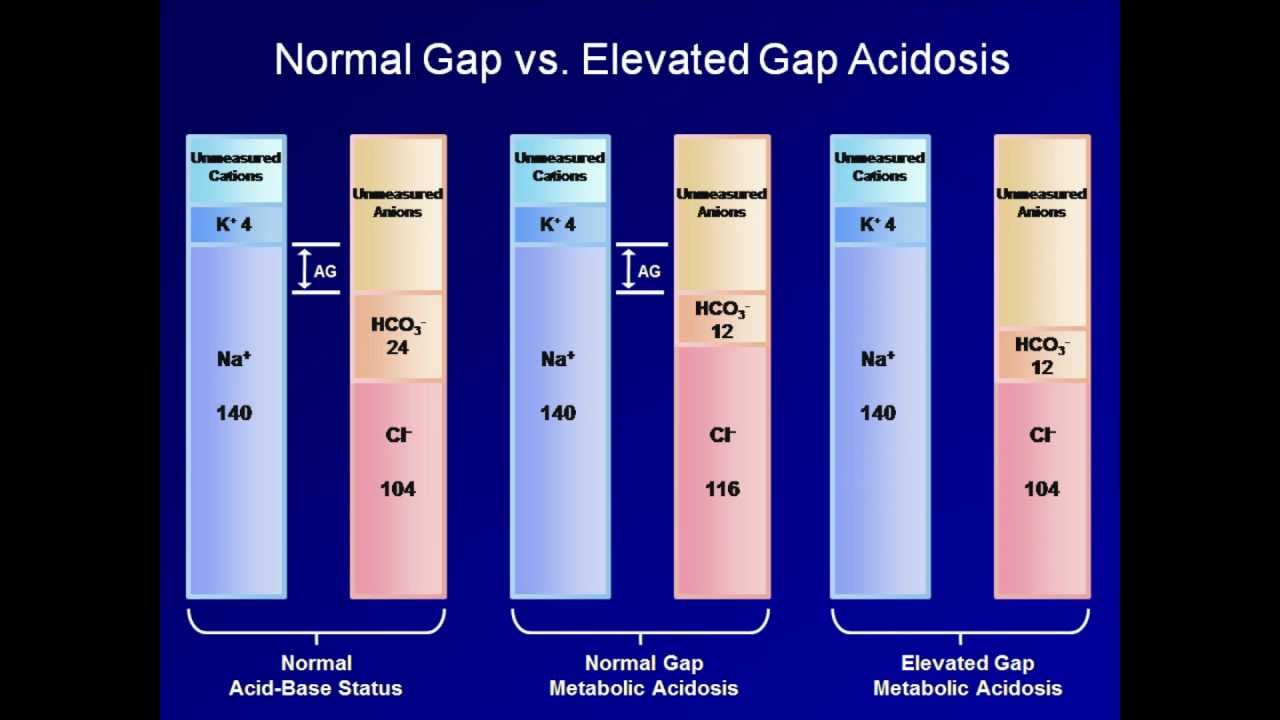
A discussion of the anion gap, including its calculation and its use in categorizing metabolic acidoses, including multiple examples of acid-base interpretation.
 0:18:57
0:18:57
ABG Interpretation: The Anion Gap (Lesson 5)
 0:58:08
0:58:08
Acid Base Disorders and ABG Interpretation | Introduction
 0:10:01
0:10:01
Plasma anion gap
 0:08:32
0:08:32
ANION GAP | Ridiculously simple
 0:42:45
0:42:45
Elevated Anion Gap Metabolic Acidosis (ABG Interpretation - Lesson 8)
 0:10:00
0:10:00
Anion Gap (AG) Calculation & Interpretation - Simply Explained
 0:21:34
0:21:34
Normal Anion Gap Metabolic Acidosis (ABG Interpretation - Lesson 9)
 0:21:14
0:21:14
ABG Interpretation: The Delta Ratio and Triple Disorders (Lesson 6)
 0:12:12
0:12:12
Anion Gap Metabolic acidosis made easy ALL YOU NEED TO KNOW
 0:06:54
0:06:54
Anion Gap EXPLAINED
 0:10:53
0:10:53
How to interpret Arterial Blood Gas (ABG) reports : Master in 10 Mins: One shot
 0:33:26
0:33:26
ABG Interpretation: A Grand Overview of Acid-Base Analysis (Lesson 13)
 0:19:17
0:19:17
ABG Interpretation: Mixed Acid-Base Disorders with Normal pH (Lesson 7)
 0:10:29
0:10:29
ABG Interpretation | Understanding Arterial Blood Gas Analysis - OSCE Guide | UKMLA | CPSA
 0:10:02
0:10:02
Respiratory Therapy - Anion Gap - When to give bicarb?
 0:22:06
0:22:06
Arterial blood gases interpretation anion gap 15/29(English)
 0:05:28
0:05:28
Acidosis and Alkalosis MADE EASY
 0:44:24
0:44:24
Respiratory Therapy - Advanced ABG Interpretations
 0:12:34
0:12:34
Medical Acid Base Balance, Disorders & ABGs Explained Clearly (Remastered)
 0:09:27
0:09:27
Delta Ratio (ABG Part - 3) | Concept and Clinical Significance.
 0:08:13
0:08:13
ABG Interpretation - Metabolic Acidosis
 0:17:12
0:17:12
ABG Interpretation: Compensation and Mixed Disorders (Lesson 4)
 0:05:02
0:05:02
Interpret an Arterial Blood gas report in 4 steps
 0:10:03
0:10:03
Arterial blood gases interpretation Urinary anion gap. 21/29(English)
Комментарии