filmov
tv
AVN Femoral Head Causes, Trauma To The Hip - Everything You Need To Know - Dr. Nabil Ebraheim

Показать описание
Dr. Ebraheim’s educational animated video describes avascular necrosis, and the of the femoral head, the signs, symptoms, diagnostic tests, prognosis.
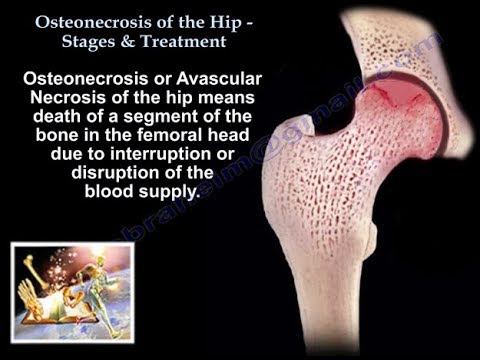
Avascular necrosis or osteonecrosis is death of a segment of bone due to disruption of the blood supply. Extraosseous or intraosseous interruption of the venous or arterial blood flow.
Mechanism of injury: fractures of the femoral neck or dislocation of the hip, mechanical disruption of the blood vessels.
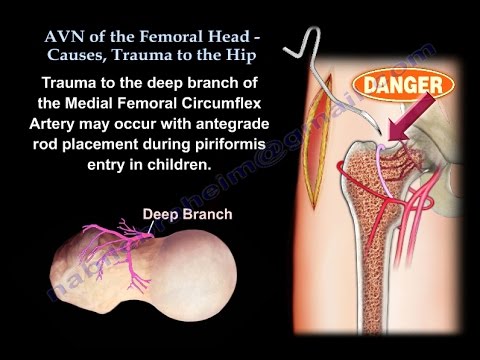
Trauma to the deep branch of the medial femoral circumflex artery may occur with antegrade rod placement during piriformis entry in children. Posterior dislocation of the femoral head should be reduced in an expedited way to decrease the risk of thrombosis of the vessels which supply the femoral head. Osteonecrosis develops in about 2-20% of hips that are reduced within 6 hours. The risk of osteonecrosis will increase with delay in reduction of the hip. Osteonecrosis appears within two years after the injury. It is evident within one year in most patients.
Pipken fracture: the patient should be informed about the complications of AVN preoperatively. Fixation failure is associated with osteonecrosis or nonunion. The affect of the anterior approach on osteonecrosis is not known. Stress fracture should be pinned before displacement occurs. Displacement will have a bad result.
Acute femoral neck fracture: nondisplaced 15% AVN, displaced and fixed properly 20-30%.
Osteonecrosis can be clinically significant when followed by lateral segmental collapse. The more vertical the fracture, the more chance that AVN will occur.
Intraoperative dissection: in acetabular fracture fixation, during intraoperative dissection for acetabular fracture reduction and fixation, avoid injury to the ascending branch of the Medial Femoral Circumflex Artery (MFCA). Fractures of the hip in children are associated with a high rate of osteonecrosis.
Four types can be identified according to Delbet classification:
Type I: Transphyseal injury 90-100% AVN.
Type II: Transcervical 50% AVN.
Type III: Cervico-trochanteric (or basicervical) 25% AVN.
Type IV: Intertrochanteric 10% AVN.
Become a friend on facebook:
Follow me on twitter:
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
Background music provided as a free download from YouTube Audio Library.
Song Title: Every Step
Avascular necrosis or osteonecrosis is death of a segment of bone due to disruption of the blood supply. Extraosseous or intraosseous interruption of the venous or arterial blood flow.
Mechanism of injury: fractures of the femoral neck or dislocation of the hip, mechanical disruption of the blood vessels.
Trauma to the deep branch of the medial femoral circumflex artery may occur with antegrade rod placement during piriformis entry in children. Posterior dislocation of the femoral head should be reduced in an expedited way to decrease the risk of thrombosis of the vessels which supply the femoral head. Osteonecrosis develops in about 2-20% of hips that are reduced within 6 hours. The risk of osteonecrosis will increase with delay in reduction of the hip. Osteonecrosis appears within two years after the injury. It is evident within one year in most patients.
Pipken fracture: the patient should be informed about the complications of AVN preoperatively. Fixation failure is associated with osteonecrosis or nonunion. The affect of the anterior approach on osteonecrosis is not known. Stress fracture should be pinned before displacement occurs. Displacement will have a bad result.
Acute femoral neck fracture: nondisplaced 15% AVN, displaced and fixed properly 20-30%.
Osteonecrosis can be clinically significant when followed by lateral segmental collapse. The more vertical the fracture, the more chance that AVN will occur.
Intraoperative dissection: in acetabular fracture fixation, during intraoperative dissection for acetabular fracture reduction and fixation, avoid injury to the ascending branch of the Medial Femoral Circumflex Artery (MFCA). Fractures of the hip in children are associated with a high rate of osteonecrosis.
Four types can be identified according to Delbet classification:
Type I: Transphyseal injury 90-100% AVN.
Type II: Transcervical 50% AVN.
Type III: Cervico-trochanteric (or basicervical) 25% AVN.
Type IV: Intertrochanteric 10% AVN.
Become a friend on facebook:
Follow me on twitter:
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
Background music provided as a free download from YouTube Audio Library.
Song Title: Every Step
 0:04:20
0:04:20
AVN Femoral Head Causes, Trauma To The Hip - Everything You Need To Know - Dr. Nabil Ebraheim
 0:11:28
0:11:28
Osteonecrosis of the Hip (femoral head) - Avascular Necrosis
 0:08:01
0:08:01
What is Avascular Necrosis (AVN)? | Why does it happen? Who gets it? How do you diagnose it?
 0:00:15
0:00:15
Check-out 👀 Hip Joint Damage from Avascular Necrosis #shorts
 0:08:13
0:08:13
Arthroscopic Treatment of Avascular Necrosis (AVN) of the Femoral Head
 0:34:29
0:34:29
AVN Femoral Head Causes, Trauma To The Hip - Everything You Need To Know
 0:04:04
0:04:04
What causes avascular necrosis of the hip (AVN)?
 0:01:12
0:01:12
Avascular necrosis of the hip and the blood supply to the femoral head.
 0:11:35
0:11:35
Avascular Necrosis of the Femoral Head #hippain #trauma #radiology
 0:06:33
0:06:33
Avascular Necrosis: Symptoms & Causes | Orthopaedic Surgeon In Bangalore -Dr JV Srinivas | Aste...
 0:13:35
0:13:35
Osteonecrosis Of The Hip Stages & Treatment - Everything You Need To Know - Dr. Nabil
 0:00:41
0:00:41
Understanding Avascular Necrosis of Hip | TOSH | Trauma and Orthopaedic Speciality Hospital
 0:03:39
0:03:39
Osteonecrosis Of The Hip Ficat Classification - Everything You Need To Know - Dr. Nabil Ebraheim
 0:03:06
0:03:06
AVN - Avascular Necrosis Breakthrough Treatment
 0:02:22
0:02:22
Explaining causes and treatments for Avascular Necrosis
 0:03:42
0:03:42
Avascular necrosis of the hip
 0:00:18
0:00:18
When Your Hip Loses 🩸 Supply - Avascular Necrosis #shorts
 0:02:08
0:02:08
Avascular Necrosis of the Hip:Explained by Paul at Ortho Eval Pal
 0:00:27
0:00:27
Common Causes For AVN Femur Head ? Dr Sai Chandra
 0:00:21
0:00:21
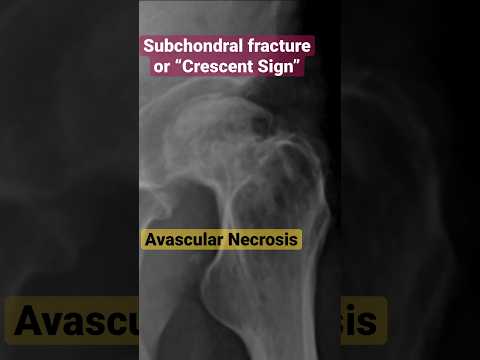
Avascular Necrosis of the Femoral Head “Crescent Sign” #xray #radiology
 0:02:53
0:02:53
Avascular Necrosis Of Femoral Head | Avascular Necrosis Diagnosis And Treatment | Bone Death | SLR
 0:04:50
0:04:50
🤷♂️What is AVN (Avascular Necrosis)? | Post Covid AVN of Femoral Head | Causes and Treatment...
 0:04:44
0:04:44
Hip AVN or Osteonecrosis: Dennis M. Lox, M.D
 0:02:10
0:02:10
What is Hip Avascular necrosis advances in treatment? - Dr. Sai Krishna Bala Krishnan Naidu
Комментарии