filmov
tv
Distal Radius fracture , Dorsal Spanning Plate - Everything You Need To Know - Dr. Nabil Ebraheim

Показать описание
Dr. Ebraheim’s educational animated video describing distal radius fractures and its fixation methods.
Fractures of the distal radius are very common constituting roughly 15% of all fractures.
Fractures are usually complicated by osteoporosis and extensive comminution of the articular surface and metaphysis.
Reconstruction is challenging and many techniques are used including plate and screws (dorsal or volar), pinning, as well as external fixation, however not all are successful with major comminution or difficult fractures.
Dorsal spanning plate application is a usual technique for these complex injuries done through a two incision approach.
This is a method we have been using for several years in difficult, select fractures and want to share our experience.
How to do it?
Surgical approach: two incisions are made:
- First incision 2-4cm centered over the dorsal aspect of the 3rd metacarpal shaft.
- Second incision is made 4-6cm over the dorsoradial aspect of the radius utilizing fluoroscopy.
- A cobb elevator is used to create a tunnel for the plate.
- The cubb is introduced through the distal incision making room for placement of the plate.
- Traction is applied to maintain reduction of the fracture.
- The plate is introduced through the developed plane and centered over the distal radial shaft.
- Care should be given to place the plate under the extensor tendons and be aware not to injury or endanger the extensor pollicis longus tendon.
- The plate is then secured to the third metacarpal shaft and to the proximal radius with screws.
- Accuracy of reduction (radial tilt inclination and height) is checked by AP and lateral C- arm view.
- Finger movements are assessed at the end of the procedure to k=make sure there is no extensor tendon entrapment.
- The plates are usually removed about 3-4 months after healing of the fracture and Physical Therapy is done to restore the wrist joint range of motion.
- The technique has proved to be useful in the management of severely comminuted fracture of the distal radius.
- The plates function like an internal/ external fixator.
Complications:
- Postoperative stiffness (most common complication).
- Extensor tendon complication including extensor pollicis longus rupture and tendon adhesions.
Become a friend on facebook:
Follow me on twitter:
Fractures of the distal radius are very common constituting roughly 15% of all fractures.
Fractures are usually complicated by osteoporosis and extensive comminution of the articular surface and metaphysis.
Reconstruction is challenging and many techniques are used including plate and screws (dorsal or volar), pinning, as well as external fixation, however not all are successful with major comminution or difficult fractures.
Dorsal spanning plate application is a usual technique for these complex injuries done through a two incision approach.
This is a method we have been using for several years in difficult, select fractures and want to share our experience.
How to do it?
Surgical approach: two incisions are made:
- First incision 2-4cm centered over the dorsal aspect of the 3rd metacarpal shaft.
- Second incision is made 4-6cm over the dorsoradial aspect of the radius utilizing fluoroscopy.
- A cobb elevator is used to create a tunnel for the plate.
- The cubb is introduced through the distal incision making room for placement of the plate.
- Traction is applied to maintain reduction of the fracture.
- The plate is introduced through the developed plane and centered over the distal radial shaft.
- Care should be given to place the plate under the extensor tendons and be aware not to injury or endanger the extensor pollicis longus tendon.
- The plate is then secured to the third metacarpal shaft and to the proximal radius with screws.
- Accuracy of reduction (radial tilt inclination and height) is checked by AP and lateral C- arm view.
- Finger movements are assessed at the end of the procedure to k=make sure there is no extensor tendon entrapment.
- The plates are usually removed about 3-4 months after healing of the fracture and Physical Therapy is done to restore the wrist joint range of motion.
- The technique has proved to be useful in the management of severely comminuted fracture of the distal radius.
- The plates function like an internal/ external fixator.
Complications:
- Postoperative stiffness (most common complication).
- Extensor tendon complication including extensor pollicis longus rupture and tendon adhesions.
Become a friend on facebook:
Follow me on twitter:
 0:01:18
0:01:18
Distal Radius Dorsal Plate
 0:03:43
0:03:43
Distal Radius fracture , Dorsal Spanning Plate - Everything You Need To Know - Dr. Nabil Ebraheim
 0:10:21
0:10:21
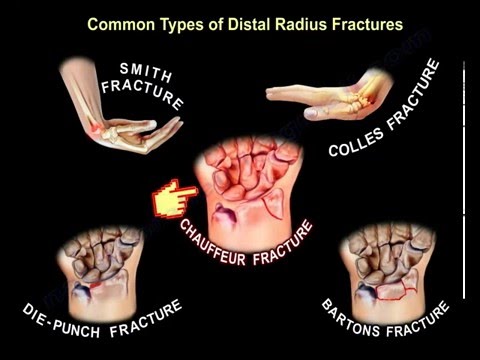
Common Types Of Distal Radius Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
 0:07:00
0:07:00
Distal Radius Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
 0:00:53
0:00:53
Distal Radius Fracture Repair
 0:10:08
0:10:08
Distal radius fractures: what to look for on radiographs
 0:03:10
0:03:10
Closed Reduction of a Distal Radius Fracture
 0:01:02
0:01:02
Distal Radius Fracture Repair - Volar Plate
 0:09:38
0:09:38
Radius, Distal - Intraarticular Fracture - Dorsal Double Plate Fixation Using VA-LCP Plates
 0:01:47
0:01:47
Distal Radius Fracture Repair
 0:00:46
0:00:46
Spanning Plate
 0:01:40
0:01:40
Distal Radius Radiographic Parameters
 0:03:27
0:03:27
How to Apply a Dorsal Backslab for Distal Radius Fractures in A&E
 0:01:14
0:01:14
Distal Radius Fracture | Jason D. Lehman, M.D.
 0:00:46
0:00:46
Surgical Fixation of Wrist Fractures
 0:08:18
0:08:18
What to expect after distal radius/wrist fractures
 0:26:40
0:26:40
Dorsal tilt, carpal malalignment & capitate shift in distal radial fractures
 0:01:30
0:01:30
Surgical Treatment of Distal Radius Fractures
 0:01:11
0:01:11
Reducing a Distal Radius Fracture
 0:01:26
0:01:26
Radial Styloid Plate Technique
 0:03:18
0:03:18
Distal Radius Fracture Therapy Exercises
 0:06:33
0:06:33
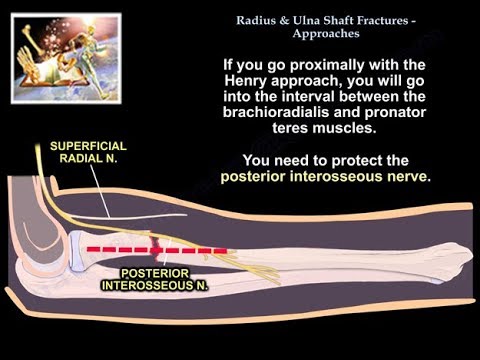
Radius & Ulnar Shaft Fracture Approaches - Everything You Need To Know - Dr. Nabil Ebraheim
 0:08:57
0:08:57
wrist fractures, symptoms, examination, diagnosis and treatment.
 0:01:04
0:01:04
Colles' Fracture Reduction Trainer
Комментарии