filmov
tv
Serratus Anterior Muscle - Everything You Need To Know - Dr. Nabil Ebraheim
Показать описание
Dr. Ebraheim’s educational animated video describes the anatomy of the Serratus Anterior muscle.
Follow me on twitter:
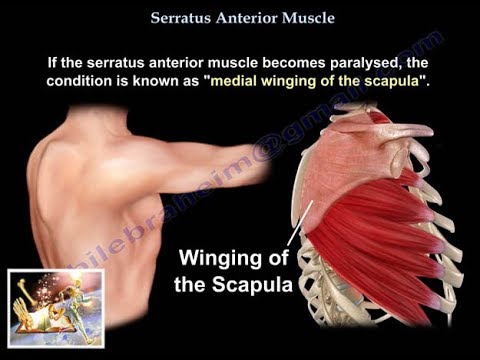
Serratus Anterior Muscle
The serratus anterior muscle originates on the superolateral surface of the upper 8 or 9 ribs. The muscle inserts into the medial border on the anterior side of the scapula. The serratus anterior muscle is divided into three parts: serratus anterior superior, serratus anterior intermediate, and serratus anterior inferior. The serratus anterior muscle is the most powerful “protractor” of the scapula. The scapula is moved laterally and anteriorly along the chest wall. The serratus anterior muscle is sometimes called the “boxer’s muscle” or the “big swing muscle”. With the same motion that occurs from throwing a punch, the serratus anterior muscle is responsible for pulling of the scapula forward and around the rib cage. The serratus anterior muscle is innervated by the long thoracic nerve. The long thoracic nerve arises from three nerve roots, C5, C6, and C7 cervical nerve roots. The long thoracic nerve then passes between the clavicle and first rib, then down along the lateral chest wall giving innervation to the serratus anterior muscle. Deficit of the serratus anterior muscle is most commonly caused due to impingement or injury of the long thoracic nerve. If the serratus anterior muscle becomes paralyzed, the condition is known as “medial winging of the scapula”. The long thoracic nerve can be injured by trauma, pressure, neuritis/inflammation, or surgery. Signs/symptoms of long thoracic nerve injury include medial winging of the scapula, difficulty elevating arm, weakness, pain, spasms (periscapular muscles trying to compensate for deformity), or cosmetic deformity. The Wall Test is used for clinical evaluation for medical winging of the scapula. The patient is asked to face a wall, standing about two feet from the wall and then push against the wall with flat palms at the waist level in order to identify a long thoracic nerve injury. The resistance of forward flexion test is also used. This is a test in which the patient resists the examiner’s attempt to bring down the forward flexed upper limbs. Lateral winging of the scapula is different from medial winging of the scapula. Lateral winging of the scapula is due to dysfunction of the trapezius muscle. Lateral scapular winging involves injury to the spinal accessory nerve. The treatment for medial scapular winging is nonoperative. Observation for a minimal of 18 months to wait for the nerve to recover without surgery. MRI to indicate if a lesion is pressing on the nerve. Muscle test and EMG or serratus anterior strengthening are also used. To treat it operatively, do a pectoralis major transfer.
Follow me on twitter:
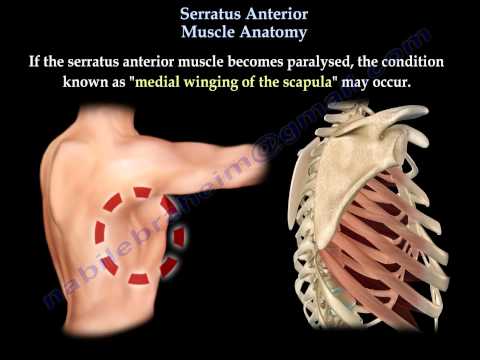
Serratus Anterior Muscle
The serratus anterior muscle originates on the superolateral surface of the upper 8 or 9 ribs. The muscle inserts into the medial border on the anterior side of the scapula. The serratus anterior muscle is divided into three parts: serratus anterior superior, serratus anterior intermediate, and serratus anterior inferior. The serratus anterior muscle is the most powerful “protractor” of the scapula. The scapula is moved laterally and anteriorly along the chest wall. The serratus anterior muscle is sometimes called the “boxer’s muscle” or the “big swing muscle”. With the same motion that occurs from throwing a punch, the serratus anterior muscle is responsible for pulling of the scapula forward and around the rib cage. The serratus anterior muscle is innervated by the long thoracic nerve. The long thoracic nerve arises from three nerve roots, C5, C6, and C7 cervical nerve roots. The long thoracic nerve then passes between the clavicle and first rib, then down along the lateral chest wall giving innervation to the serratus anterior muscle. Deficit of the serratus anterior muscle is most commonly caused due to impingement or injury of the long thoracic nerve. If the serratus anterior muscle becomes paralyzed, the condition is known as “medial winging of the scapula”. The long thoracic nerve can be injured by trauma, pressure, neuritis/inflammation, or surgery. Signs/symptoms of long thoracic nerve injury include medial winging of the scapula, difficulty elevating arm, weakness, pain, spasms (periscapular muscles trying to compensate for deformity), or cosmetic deformity. The Wall Test is used for clinical evaluation for medical winging of the scapula. The patient is asked to face a wall, standing about two feet from the wall and then push against the wall with flat palms at the waist level in order to identify a long thoracic nerve injury. The resistance of forward flexion test is also used. This is a test in which the patient resists the examiner’s attempt to bring down the forward flexed upper limbs. Lateral winging of the scapula is different from medial winging of the scapula. Lateral winging of the scapula is due to dysfunction of the trapezius muscle. Lateral scapular winging involves injury to the spinal accessory nerve. The treatment for medial scapular winging is nonoperative. Observation for a minimal of 18 months to wait for the nerve to recover without surgery. MRI to indicate if a lesion is pressing on the nerve. Muscle test and EMG or serratus anterior strengthening are also used. To treat it operatively, do a pectoralis major transfer.
Serratus Anterior Muscle - Everything You Need To Know - Dr. Nabil Ebraheim
 0:02:41
0:02:41
Serratus Anterior Muscle: Function, Origins - Human Anatomy | Kenhub
 0:00:37
0:00:37
Serratus Anterior Training (🥊Boxer's Muscle)
 0:00:40
0:00:40
The Serratus Anterior Muscle
 0:04:53
0:04:53
Serratus Anterior Muscle Anatomy, winged scapula - Everything You Need To Know - Dr. Nabil Ebraheim
 0:02:39
0:02:39
The serratus anterior
 0:00:17
0:00:17
Back muscles: Anatomy of serratus #shorts
 0:03:41
0:03:41
Serratus Anterior Anatomy: Origin, Insertion & Action
 0:00:14
0:00:14
serratus anterior #serratusanterior #anatomy #skeleton #muscles #biomechanics #scapula
 0:09:24
0:09:24
How To “Sculpt” Your Serratus Anterior (STOP Neglecting This Muscle!)
 0:00:32
0:00:32
3 Exercises To Strengthen Your Serratus
 0:14:37
0:14:37
You NEED to Train This Overlooked Muscle: Serratus Anterior
 0:00:44
0:00:44
The Key To Unlocking Your Serratus Anterior Muscle For Shoulder Health #shoulderpain #fitness #gym
 0:00:59
0:00:59
Avoid These Serratus Anterior Mistakes!
 0:00:18
0:00:18
Serratus Anterior Muscle Activation Exercise
 0:06:18
0:06:18
7 Great Serratus Anterior & Posterior Exercises
 0:00:34
0:00:34
serratus anterior muscle! #anatomy
 0:00:15
0:00:15
Movements to help you bring relief to your scapular region 👁 #scapularmobility #scapulamobility
 0:05:01
0:05:01
Serratus anterior muscle
 0:02:07
0:02:07
Serratus Anterior: Shoulder Series, Part 11 (3D Animation)
 0:06:04
0:06:04
Serratus Anterior Muscle Anatomy | Muscle of Pectoral Region | Doctor Speaks
 0:00:30
0:00:30
YOU NEED to Exercise your Serratus Anterior for Shoulder Health!
 0:00:26
0:00:26
How to TRAIN your Serratus Anterior! #shorts
 0:00:57
0:00:57
Serratus Anterior Exercise
Комментарии