filmov
tv
WEIGHT LOSS SURGERY REVISIONS | Reoperation after Bariatric Surgery

Показать описание
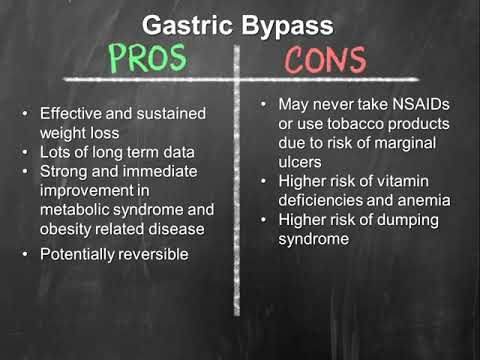
Dr. Blaney is talking about re-operation after weight loss surgery. This is occasionally required when patients experience unsatisfactory weight loss or weight regain. However there can be complications or side effects that might necessitate converting or revising a previously preformed bariatric procedure.
 0:04:19
0:04:19
WEIGHT LOSS SURGERY REVISIONS | Reoperation after Bariatric Surgery
 0:01:16
0:01:16
Weight-loss revision surgery
 0:02:59
0:02:59
Revision Bariatric Surgery: Janice's Weight-Loss Journey
 0:10:24
0:10:24
Types of Weight Loss Surgery | OSF Saint Francis Medical Center
 0:04:42
0:04:42
All About Weight Loss Surgery Revisions
 0:03:58
0:03:58
Bariatric Revision Surgery
 0:09:19
0:09:19
What you need to know about Revision Weight Loss Surgery by Dr Arun Dhir
 0:12:00
0:12:00
Bariatric Surgery Revisions
 0:01:40
0:01:40
Gastric Bypass Surgery - Nina's Story | Temple Bariatric Program
 0:02:22
0:02:22
Bariatric Revision after gastric bypass
 0:02:19
0:02:19
Bariatric Revision after gastric bypass surgery! Non surgical, endoscopic solution #TORe
 0:02:29
0:02:29
COST OF REVISIONS | Is There a Discount for My Weight Loss Surgery Revision?
 0:02:21
0:02:21
Revision Bariatric Surgery with Dallas Weight Loss Surgeon Dr. Daryl Stewart
 0:01:12
0:01:12
Endoscopic Revision of Sleeve Gastrectomy: explained
 0:03:18
0:03:18
Revision surgery for weight regain after sleeve gastrectomy
 0:01:43
0:01:43
Which bariatric surgery is safest and most effective?
 0:02:06
0:02:06
Bariatric Weight Loss Revision Surgery with Dr. Jason Payne
 0:01:11
0:01:11
Revision Bariatric / Weight Loss Surgery
 0:04:51
0:04:51
Why You May Need to Convert or Revise a Bariatric Procedure
 0:01:44
0:01:44
Revision Weight Loss Surgery
 0:01:25
0:01:25
Endoscopic Gastric Bypass revision (Transoral Gastric Outlet Reduction): How does it work?
 0:02:00
0:02:00
Bariatric Revision after gastric sleeve
 0:00:54
0:00:54
Main reasons for revision bariatric surgery
 0:01:44
0:01:44
Gastric Bypass Revision Animation, Grand Strand Bariatric Surgery
Комментарии