filmov
tv
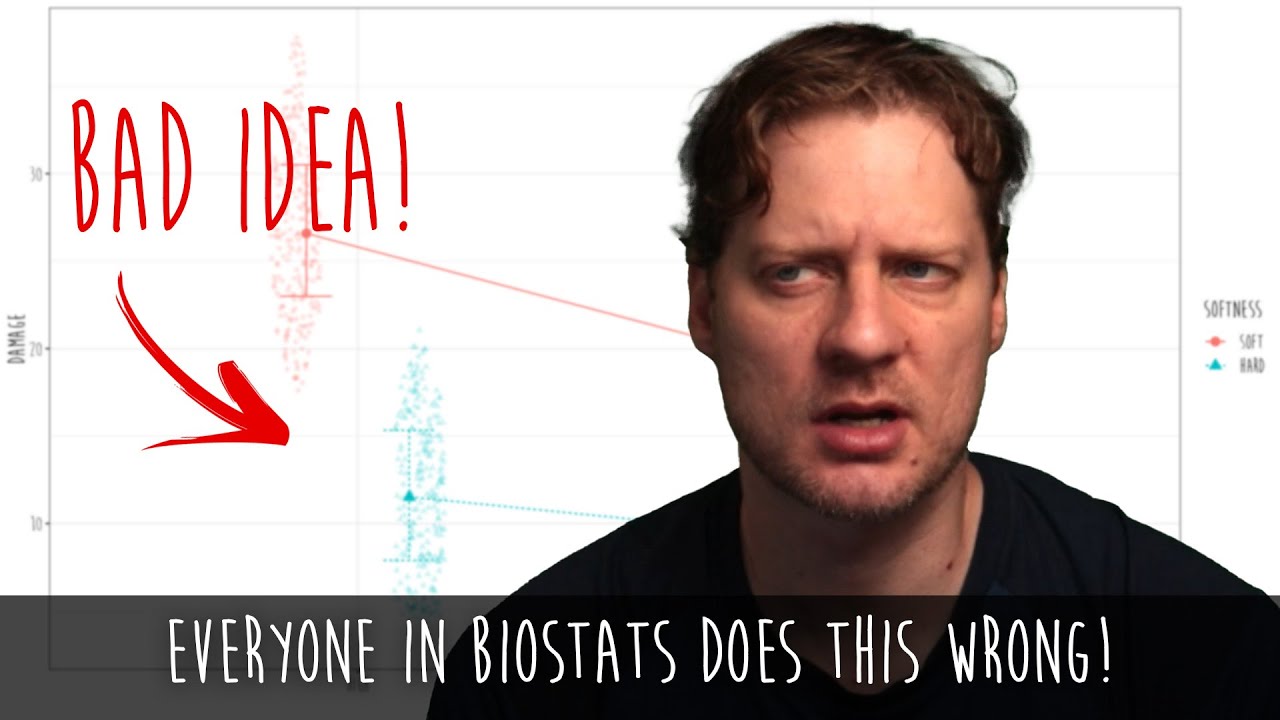
The most common mistake in biostatistics
Показать описание
*Technical side note: zero-inflated simply means you have a distribution with an abnormal number of zeroes. To model zero-inflated data, it's common to use models that combine logistic regression (to predict the 0 vs 1) and logistic regression (to predict 1+). So it's technically incorrect to say that a distribution that has this characteristic (combining yes/no with degree) is "zero-inflated." In other words, zero-inflated describes the distribution, not how the distribution is modeled. Make sense?
 0:18:22
0:18:22
7 Most Common English Grammar Mistakes + TEST - Do you make these mistakes?
 0:00:17
0:00:17
The Most Common Mistake In Pool
 0:00:33
0:00:33
Most Common MISTAKE In Chess
 0:02:24
0:02:24
The Most Common Mistake in Hamster Kombat 🐹 Hamster Academy
 0:09:49
0:09:49
5 Very Common Grammatical Mistakes In English
 0:00:27
0:00:27
The Most Common MISTAKE in Diamond...
 0:00:35
0:00:35
99% People Make This☝️ Common Mistake in English | English Speaking Practice #englishmistakes #learn...
 0:17:51
0:17:51
The Most Common Mistake In Sim Racing
 0:29:53
0:29:53
3D Bloom Art: The Most Common Mistakes
 0:24:59
0:24:59
10 Grammar Mistakes You Make When You Speak English
 0:01:00
0:01:00
The MOST COMMON mistake in Minecraft! 🏓 #shorts
 0:00:55
0:00:55
This is the most common mistake people make in marketing
 0:00:32
0:00:32
THE most COMMON Mistake in #english #learnenglish #ingles
 0:13:56
0:13:56
FREESTYLE SWIMMING: 5 MOST COMMON MISTAKES
 0:22:50
0:22:50
50 MOST COMMON MISTAKES in English Grammar - Error Identification & Correction
 0:00:35
0:00:35
The Most Common Pie Dough Mistake
 0:00:24
0:00:24
The Most Common Mistake in R6...
 0:07:40
0:07:40
The Most Common Mistake in Bowling
 0:21:39
0:21:39
The Most Common Mistakes in English | Don't Make These Speaking Mistakes!
 0:11:33
0:11:33
Are You Making These Mistakes In English Grammar?
 0:00:53
0:00:53
Most Common Mistake
 0:00:45
0:00:45
The Most Common Mistake in CODM😭
 0:37:17
0:37:17
7 MOST COMMON Chess Mistakes
 0:13:00
0:13:00
10 Most Common English Grammar Mistakes || Basic English Grammar
Комментарии