filmov
tv
nerve injury of the upper and lower extremity, complete easy review of nerve injuries

Показать описание
1- long thoracic nerve: medial winging of the scapula is most commonly caused by deficit in the serratus anterior muscle due to impingement of the long thoracic nerve.
2- Median nerve injury: carpal tunnel syndrome: inflammation of the carpal tunnel compresses the median nerve and causes tingling, numbness, weakness, or pain in the thumb, index finger, middle finger, and half of the ring finger. Surgical release of the carpal tunnel is needed.
3- Ulnar nerve injury: cubital tunnel syndrome: pressure on the nerve at the elbow can cause numbness or pain in the elbow, hand, wrist, or fingers. Compression of the ulnar nerve below the elbow may lead to claw hand.
4- Posterior interosseous nerve injury: at about the level of the lateral epicondyle, the radial nerve begins to divided into the deep branch and the superficial branch of the radial nerve. The posterior interosseous nerve (deep) enters the extensor compartment of the forearm through the supinator muscle. The posterior interosseous nerve supplies these muscles on the radial side and dorsal surface of the forearm. The posterior interosseous nerve does not supply cutaneous sensation and is purely a motor nerve. Entrapment at the Arcade of Frohse: with injury to the posterior interosseous nerve, the patient will experience difficulty with extension of the fingers only.
5- Anterior interosseous nerve injury: about half the way down the forearm, the anterior interosseous nerve exits from the dorsal lateral aspect of the median nerve. The anterior interosseous nerve is purely motor. All the muscles in front of the forearm are supplied by the median nerve except the medial half of the flexor digitorum profundus. The anterior interosseous nerve gives branches to three muscles: Pronator quadratus, lateral half of the flexor digitorum profundus, flexor pollicis longus. The patient will be unable to give the OK sign due to paralysis of the flexor pollicis longus and the flexor digitorum profundus.
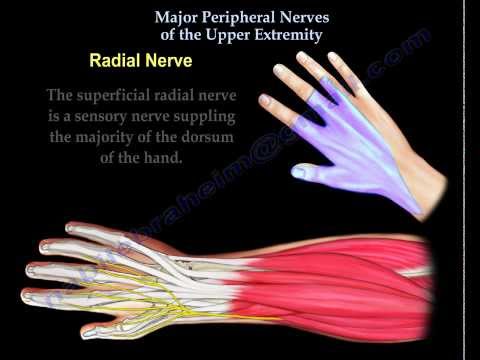
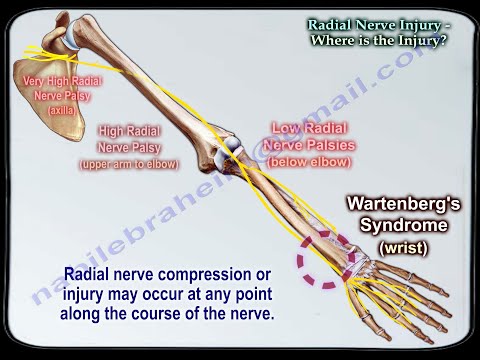
6- Radial nerve injury: radial nerve compression or injury may occur at any point along the course of the nerve.
7- Axillary nerve injury: the axillary nerve supplies the deltoid muscles, giving sensation over the shoulder area. The axillary nerve originates from the posterior cord of the brachial plexus. When the nerve is injured: weakness of shoulder abduction, atrophy of the deltoid, numbness in the deltoid region. The axillary nerve is commonly injured due to fractures or dislocations of the shoulder joint.
8- Femoral nerve injury: the muscles of the anterior compartment of the thigh are innervated by the femoral nerve. The usual cause of femoral nerve dysfunction are due to trauma or compression of the nerve. The quadriceps tendon is a strong tendon which groups the four muscles that extend the knee: rectus femoris, vastus intermedius (under rectus femoris), vastus medialis, vastus laterlaris.
Differential diagnosis: tears of the quadriceps tendon, patellar tendon injury or patellar fractures cause an inability to extend the knee. A quadriceps tendon rupture is rupture of the tendon that inserts into the top of the patella.
9- Posterior tibial nerve injury: the tarsal tunnel is located just below the medial malleolus of the ankle and is covered with a thick band of ligaments called the flexor retinaculum. The flexor retinaculum protect the structures contained within the tunnel such as the posterior tibial nerve. The structures which also pass through the tunnel include the posterior tibial artery, the tendons of the tibialis posterior, flexor digitorum longus, and the flexor hallucis longus. Tarsal tun el syndrome is a compression neuropathy caused by compression of the posterior tibial nerve within the tarsal tunnel. With tarsal tunnel syndrome there will be pain and numbness on the plantar aspect of the foot and heel. Tibial nerve compression with tarsal tunnel syndrome is similar to carpal tunnel syndrome which occurs at the wrist.
10- Common peroneal nerve injury: the ankle and foot dorsiflexors are supplied by the peroneal nerve which is part of the sciatic nerve. The sciatic nerve starts in the lower back and runs through the buttock and lower limb. In the lower thigh, just above the back of the knee, the sciatic nerve divides into two nerves, the tibial and the peroneal nerves, which innervate different parts of the lower leg. The common peroneal nerve then travels anterior, around the fibular neck, dividing into superficial and deep peroneal nerves. The deep peroneal nerve gives innervation to the tibialis anterior muscle of the lower leg which is responsible for dorsiflexion of the ankle. Conditions causing foot drop: injury to the knee: knee dislocation: in the event of knee dislocation, it is important to check for common peroneal nerve and popliteal artery injury.
Become a friend on facebook:
Follow me on twitter:
2- Median nerve injury: carpal tunnel syndrome: inflammation of the carpal tunnel compresses the median nerve and causes tingling, numbness, weakness, or pain in the thumb, index finger, middle finger, and half of the ring finger. Surgical release of the carpal tunnel is needed.
3- Ulnar nerve injury: cubital tunnel syndrome: pressure on the nerve at the elbow can cause numbness or pain in the elbow, hand, wrist, or fingers. Compression of the ulnar nerve below the elbow may lead to claw hand.
4- Posterior interosseous nerve injury: at about the level of the lateral epicondyle, the radial nerve begins to divided into the deep branch and the superficial branch of the radial nerve. The posterior interosseous nerve (deep) enters the extensor compartment of the forearm through the supinator muscle. The posterior interosseous nerve supplies these muscles on the radial side and dorsal surface of the forearm. The posterior interosseous nerve does not supply cutaneous sensation and is purely a motor nerve. Entrapment at the Arcade of Frohse: with injury to the posterior interosseous nerve, the patient will experience difficulty with extension of the fingers only.
5- Anterior interosseous nerve injury: about half the way down the forearm, the anterior interosseous nerve exits from the dorsal lateral aspect of the median nerve. The anterior interosseous nerve is purely motor. All the muscles in front of the forearm are supplied by the median nerve except the medial half of the flexor digitorum profundus. The anterior interosseous nerve gives branches to three muscles: Pronator quadratus, lateral half of the flexor digitorum profundus, flexor pollicis longus. The patient will be unable to give the OK sign due to paralysis of the flexor pollicis longus and the flexor digitorum profundus.
6- Radial nerve injury: radial nerve compression or injury may occur at any point along the course of the nerve.
7- Axillary nerve injury: the axillary nerve supplies the deltoid muscles, giving sensation over the shoulder area. The axillary nerve originates from the posterior cord of the brachial plexus. When the nerve is injured: weakness of shoulder abduction, atrophy of the deltoid, numbness in the deltoid region. The axillary nerve is commonly injured due to fractures or dislocations of the shoulder joint.
8- Femoral nerve injury: the muscles of the anterior compartment of the thigh are innervated by the femoral nerve. The usual cause of femoral nerve dysfunction are due to trauma or compression of the nerve. The quadriceps tendon is a strong tendon which groups the four muscles that extend the knee: rectus femoris, vastus intermedius (under rectus femoris), vastus medialis, vastus laterlaris.
Differential diagnosis: tears of the quadriceps tendon, patellar tendon injury or patellar fractures cause an inability to extend the knee. A quadriceps tendon rupture is rupture of the tendon that inserts into the top of the patella.
9- Posterior tibial nerve injury: the tarsal tunnel is located just below the medial malleolus of the ankle and is covered with a thick band of ligaments called the flexor retinaculum. The flexor retinaculum protect the structures contained within the tunnel such as the posterior tibial nerve. The structures which also pass through the tunnel include the posterior tibial artery, the tendons of the tibialis posterior, flexor digitorum longus, and the flexor hallucis longus. Tarsal tun el syndrome is a compression neuropathy caused by compression of the posterior tibial nerve within the tarsal tunnel. With tarsal tunnel syndrome there will be pain and numbness on the plantar aspect of the foot and heel. Tibial nerve compression with tarsal tunnel syndrome is similar to carpal tunnel syndrome which occurs at the wrist.
10- Common peroneal nerve injury: the ankle and foot dorsiflexors are supplied by the peroneal nerve which is part of the sciatic nerve. The sciatic nerve starts in the lower back and runs through the buttock and lower limb. In the lower thigh, just above the back of the knee, the sciatic nerve divides into two nerves, the tibial and the peroneal nerves, which innervate different parts of the lower leg. The common peroneal nerve then travels anterior, around the fibular neck, dividing into superficial and deep peroneal nerves. The deep peroneal nerve gives innervation to the tibialis anterior muscle of the lower leg which is responsible for dorsiflexion of the ankle. Conditions causing foot drop: injury to the knee: knee dislocation: in the event of knee dislocation, it is important to check for common peroneal nerve and popliteal artery injury.
Become a friend on facebook:
Follow me on twitter:
 0:03:43
0:03:43
Nerve injury of the upper extremity - Everything You Need To Know - Dr. Nabil Ebraheim
 0:08:20
0:08:20
Upper Extremity Nerve Injuries
 0:10:16
0:10:16
NERVE INJURY IN THE UPPER EXTREMITY- Common nerve injuries in the upper extremity
 0:03:59
0:03:59
Quick & Easy Upper Limb Nerve Tests | Radial, Median, Ulna, AIN Nerves: Rock, Paper, Scissors, O...
 0:07:56
0:07:56
Median, Ulnar, Radial Nerve Injuries | Simple Tricks | OT MIRI
 0:08:12
0:08:12
Nerve Injury Signs | Expert Explains Wartenburgs, Froments, Ulnar Claw, Hand of Benediction, OK Sign
 0:13:04
0:13:04
nerve injury of the upper and lower extremity, complete easy review of nerve injuries
 0:01:21
0:01:21
Treating nerve damage in hands or upper arms | Ohio State Medical Center
 0:06:05
0:06:05
5 Min Yoga for Lower Back Pain l Say GOODBYE to Lower Back Pain with YOGA! l Back Pain relief l
 0:05:42
0:05:42
Nerve Injuries: Median Nerve – MRCS | Lecturio
 0:35:26
0:35:26
Neurology | Nerve Injury & Repair: Wallerian Degeneration & Regeneration
 0:06:00
0:06:00
Upper Limb Nerve Injuries (Made Easy) || USMLE
 0:07:58
0:07:58
Radial Nerve Injury,Where Is The Injury - Everything You Need To Know - Dr. Nabil Ebraheim
 0:00:51
0:00:51
Instant Upper Back and Neck Pain Relief #Shorts
 0:00:50
0:00:50
Relieve Carpal Tunnel Syndrome in Seconds #Shorts
 0:00:55
0:00:55
Quick Nerve Pain Relief in Neck and Shoulder
 0:01:20
0:01:20
Nerve Injuries in The Upper Limb | All about the Upper Limb | Dr. Warid Altaf | Sancheti Hospital
 0:44:20
0:44:20
𝟐𝟏. 𝐍𝐞𝐫𝐯𝐞 𝐢𝐧𝐣𝐮𝐫𝐢𝐞𝐬 𝐨𝐟 𝐭𝐡𝐞 𝐮𝐩𝐩𝐞𝐫 𝐥𝐢𝐦𝐛 (𝐂𝐚𝐮𝐬𝐞𝐬 𝐚𝐧𝐝 𝐜𝐥𝐢𝐧𝐢𝐜𝐚𝐥 𝐩𝐢𝐜𝐭𝐮𝐫𝐞)...
 0:00:12
0:00:12
Training 💪 After Brachial Plexus Nerve Injury #shorts
 0:08:07
0:08:07
Nerve Compressions Of The Upper Extremity - Everything You Need To Know - Dr. Nabil Ebraheim
 0:00:55
0:00:55
Instant Relief for Pinched Nerve Pain in the Back and Leg
 0:00:59
0:00:59
Pinched Nerve In Your Neck? These Two Exercises Can Help FAST!
 0:00:55
0:00:55
Ulnar Paradox #physicaltherapy #physiotherapy #ulnarnerve #ulnarclaw #anatomy
 0:08:28
0:08:28
Upper Extremity Nerve Injury | MSK | Step 1 Simplified
Комментарии