filmov
tv
Chocolate Ovarian Cyst versus the Hemorrhagic Ovarian Cyst.

Показать описание
This video shows Chocolate Ovarian Cyst versus the Hemorrhagic Ovarian Cyst.
Chocolate cysts are noncancerous, fluid-filled cysts that typically form deep within the ovaries. They're also called ovarian endometriomas. The color comes from old menstrual blood and tissue that fills the cavity of the cyst. A chocolate cyst can affect one or both ovaries and may occur in multiples or singularly.
A hemorrhagic ovarian cyst (HOC) is an adnexal mass formed because of the occurrence of bleeding into a follicular or corpus luteum cyst. Hemorrhagic cysts are commonly seen in clinical practice because hemorrhage into a cyst is usually painful, triggering the patient to consult her physician.
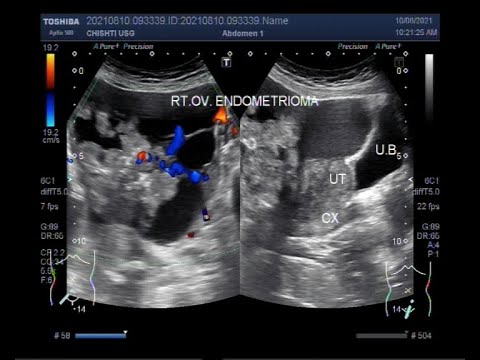
Endometrioma is distinguished from other types of ovarian cysts by a somewhat grainy and not completely anechoic content.
Endometriosis causes chocolate cysts. Endometrial tissue lines the uterus, and endometriosis causes this tissue to grow outside the uterus as well. Endometrial tissue can attach to the ovaries, fallopian tubes, and nearby organs, such as the bladder.
An ovarian cyst is a fluid-filled sac that develops in or on the ovary and usually disappears after ovulation. Most ovarian cysts don't cause any problems and go away on their own.
Chocolate cysts are common in women with endometriosis. Symptoms can often be managed with medication. In some cases, the cysts will need to be removed. According to a study, about 30 percent of surgically removed chocolate cysts will return, especially if they were large or medically treated.
If ovulation occurs less often, or if the eggs are less healthy, the chances of pregnancy decrease. It is important to remember that endometriomas do not inevitably cause infertility. In fact, some women with advanced endometriosis and chocolate cysts easily get pregnant.
Endometriomas may be considered the most serious threat to a woman's reproductive potential, with the exception of cancerous tumors of the reproductive tract. These cysts can represent a medical dilemma even while women are receiving fertility treatments such as assisted reproductive technologies (ART).
Hemorrhagic ovarian cysts
A hemorrhagic ovarian cyst (HOC) is an adnexal mass formed because of the occurrence of bleeding into a follicular or corpus luteum cyst. Hemorrhagic cysts are commonly seen in clinical practice because hemorrhage into a cyst is usually painful, triggering the patient to consult her physician.
Many radiologists use the term “complex” to describe all cysts other than totally clear, simple cysts. However, many benign entities are complex, such as dermoid cysts, endometriomas, hemorrhagic cysts, and cystadenomas.
Having a hemorrhagic ovarian cyst is not necessarily a problem. Many times these cysts don't cause symptoms and are often found during a pelvic exam that's done for another reason. If a cyst is small or medium-size and isn't causing you any pain or other symptoms, then your doctor likely will recommend monitoring it.
A hemorrhagic or a ruptured ovarian cyst is the most common cause of acute pelvic pain in an afebrile, premenopausal woman presenting to the emergency room. They can occur during pregnancy.
Hemorrhagic cysts are normal in ovulatory women, usually resolving within 8 weeks. They can be quite variable in appearance, however, and can be confused with ovarian endometriomas.
In addition to pain, symptoms of a ruptured ovarian cyst can include:
bleeding from the vagina.
nausea.
vomiting.
tenderness in the pelvic/abdominal area.
weakness.
feeling faint.
fever.
increased pain while sitting.
Ovarian cysts are fluid-filled sacs that can develop in or on a person's ovaries. The cysts are usually benign, which means they are not cancerous and often clear up without treatment.
Having a cyst on an ovary does not usually affect one's chances of becoming pregnant, which is why doctors will typically only investigate further if a couple has been trying to conceive naturally through regular intercourse for a year, but has not yet been successful in falling pregnant.
Chocolate cysts are noncancerous, fluid-filled cysts that typically form deep within the ovaries. They're also called ovarian endometriomas. The color comes from old menstrual blood and tissue that fills the cavity of the cyst. A chocolate cyst can affect one or both ovaries and may occur in multiples or singularly.
A hemorrhagic ovarian cyst (HOC) is an adnexal mass formed because of the occurrence of bleeding into a follicular or corpus luteum cyst. Hemorrhagic cysts are commonly seen in clinical practice because hemorrhage into a cyst is usually painful, triggering the patient to consult her physician.
Endometrioma is distinguished from other types of ovarian cysts by a somewhat grainy and not completely anechoic content.
Endometriosis causes chocolate cysts. Endometrial tissue lines the uterus, and endometriosis causes this tissue to grow outside the uterus as well. Endometrial tissue can attach to the ovaries, fallopian tubes, and nearby organs, such as the bladder.
An ovarian cyst is a fluid-filled sac that develops in or on the ovary and usually disappears after ovulation. Most ovarian cysts don't cause any problems and go away on their own.
Chocolate cysts are common in women with endometriosis. Symptoms can often be managed with medication. In some cases, the cysts will need to be removed. According to a study, about 30 percent of surgically removed chocolate cysts will return, especially if they were large or medically treated.
If ovulation occurs less often, or if the eggs are less healthy, the chances of pregnancy decrease. It is important to remember that endometriomas do not inevitably cause infertility. In fact, some women with advanced endometriosis and chocolate cysts easily get pregnant.
Endometriomas may be considered the most serious threat to a woman's reproductive potential, with the exception of cancerous tumors of the reproductive tract. These cysts can represent a medical dilemma even while women are receiving fertility treatments such as assisted reproductive technologies (ART).
Hemorrhagic ovarian cysts
A hemorrhagic ovarian cyst (HOC) is an adnexal mass formed because of the occurrence of bleeding into a follicular or corpus luteum cyst. Hemorrhagic cysts are commonly seen in clinical practice because hemorrhage into a cyst is usually painful, triggering the patient to consult her physician.
Many radiologists use the term “complex” to describe all cysts other than totally clear, simple cysts. However, many benign entities are complex, such as dermoid cysts, endometriomas, hemorrhagic cysts, and cystadenomas.
Having a hemorrhagic ovarian cyst is not necessarily a problem. Many times these cysts don't cause symptoms and are often found during a pelvic exam that's done for another reason. If a cyst is small or medium-size and isn't causing you any pain or other symptoms, then your doctor likely will recommend monitoring it.
A hemorrhagic or a ruptured ovarian cyst is the most common cause of acute pelvic pain in an afebrile, premenopausal woman presenting to the emergency room. They can occur during pregnancy.
Hemorrhagic cysts are normal in ovulatory women, usually resolving within 8 weeks. They can be quite variable in appearance, however, and can be confused with ovarian endometriomas.
In addition to pain, symptoms of a ruptured ovarian cyst can include:
bleeding from the vagina.
nausea.
vomiting.
tenderness in the pelvic/abdominal area.
weakness.
feeling faint.
fever.
increased pain while sitting.
Ovarian cysts are fluid-filled sacs that can develop in or on a person's ovaries. The cysts are usually benign, which means they are not cancerous and often clear up without treatment.
Having a cyst on an ovary does not usually affect one's chances of becoming pregnant, which is why doctors will typically only investigate further if a couple has been trying to conceive naturally through regular intercourse for a year, but has not yet been successful in falling pregnant.
 0:04:03
0:04:03
Chocolate Ovarian Cyst versus the Hemorrhagic Ovarian Cyst.
 0:06:58
0:06:58
What Is Chocolate Cyst? | Chocolate Cyst/ Endometriosis Cyst Pregnancy Chances
 0:12:59
0:12:59
What Is Chocolate Cyst? | Chocolate Cyst (Ovarian Endometrioma) | Cause | Symptoms | Treatment
 0:02:44
0:02:44
Large Ovarian Endometrioma, also known as a chocolate cyst or Endometriotic cyst.
 0:02:08
0:02:08
How are Chocolate cysts dealt? - Dr. Sunil Eshwar
 0:05:00
0:05:00
Large Ovarian Endometrioma, also known as chocolate cyst or Endometriotic cyst.
 0:06:19
0:06:19
Chocolate Cysts and Ovarian Reserve
 0:02:27
0:02:27
Hemorrhagic vs Endometriotic vs Dermoid cyst -Recap series V2
 0:02:46
0:02:46
Ovarian Cysts: Causes, Symptoms & Natural Treatment – Dr.Berg
 0:03:45
0:03:45
Chocolate Ovarian Cyst also known as Endometriomas.
 0:11:32
0:11:32
Ovarian cysts in women : Symptoms | Causes | Diagnosis | Treatment | Dr Rooma Sinha
 0:06:55
0:06:55
Chocolate Cyst In Ovary (endometriosis) Cause Symptoms and Treatments
 0:04:48
0:04:48
Endometriomas, also known as chocolate cysts or endometriotic cysts.
 0:01:30
0:01:30
What Can Cause Ovarian Cysts?
 0:01:39
0:01:39
Signs and Symptoms of Ovarian Cysts
 0:00:13
0:00:13
Ovarian Hemorrhagic cyst and endometrioma cyst in patient with irregular bleeding/period .
 0:04:48
0:04:48
Ovarian Endometrioma, Endometriosis, Pain and Infertility.
 0:04:10
0:04:10
Ultrasound Video showing a Chocolate ovarian cyst and a hemorrhagic ovarian cyst.
 0:01:45
0:01:45
What types of ovarian cysts are cancerous?
 0:00:35
0:00:35
Why is the ovarian cyst called chocolate cyst?
 0:03:04
0:03:04
Ultrasound Video showing difference between the simple and hemorrhagic ovarian cysts.
 0:06:58
0:06:58
Endometriosis or chocolate cyst in females ovary - IRCC Pakistan
 0:03:54
0:03:54
Just 3 Recommendations To Cure Ovarian Cyst Naturally - Dr. Vivek Joshi
 0:00:50
0:00:50
High Yielding Shorts-13 (#HYS-13) : Chocolate Cyst (Ovarian Endometriosis) by Dr. Devesh Mishra.
Комментарии