filmov
tv
Anatomy Of The Subscapularis Muscle - Everything You Need To Know - Dr. Nabil Ebraheim
Показать описание
The subscapularis muscle is a large muscle that originates on the anterior surface of the scapula and lies in front of the shoulder. The muscle passes to its insertion into the humeral head underneath the arch formed by the coracoid process and the combined origins of the coracobrachialis muscle and short head of the biceps.
The subscapularis muscles is the largest of the four rotator cuff muscles and it provides about 50% of the total cuff strength.
The subscapularis muscles insert into the lesser tuberosity of the humerus, while the other rotator cuff muscles have an insertion into the greater tuberosity.
The subscapularis muscle acts as a dynamic stabilizer of the humeral head and aids in lifting across the chest. The function of the subscapularis muscle is to adduct and rotate the arm medially.
Posterior dislocation of the humeral head with a “reverse Hills-Sachs lesion” is a rare condition. the condition can be repaired after reduction of the dislocation with the McLaughlin procedure utilizing the subscapularis tendon if the lesion is between 20-40 of the humeral head. The subscapularis tendon is used to fill the reverse Hill-Sachs lesion using suture anchors or screws inserted in the humeral head defect. The screws are inserted into a portion of the lesser tuberosity that is attached to the subscapularis.
At the insertion of the subscapularis tendon into the humerus lies the transverse humeral ligament. the long head of the biceps tendon lies within the bicipital groove and is held in place by the transverse humeral ligament. when a complete rupture of the subscapularis tendon occurs, the transverse humeral ligament may also become torn causing medial dislocation of the biceps tendon from the bicipital groove.
Radiological examination
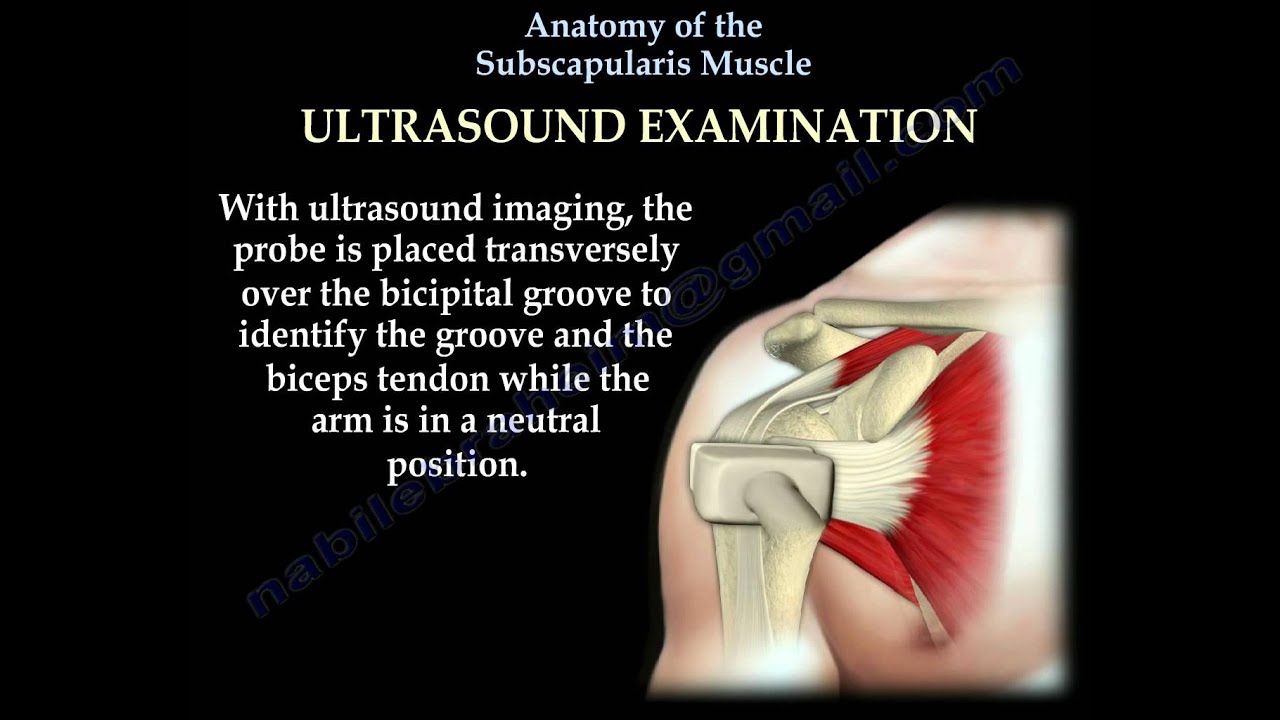
•Tears of the subscapularis tendon may be diagnosed by using MRI or ultrasound.
•With ultrasound imaging, the probe is placed transversely over the bicipital groove to identify the groove and the biceps tendon while the arm is in a neutral position. The arm is then externally rotated to view the subscapularis tendon.
Diagnosis of the subscapularis rupture
Tears are not common and can be occult. Can be either chronic or acute.
Patient will have
•Pain
•Anterior shoulder swelling
•Decreased range of motion
•The weakness of internal rotation.
Lift-off test
The patient places the hand behind their back at the lumbar level and lifts the hand away form the back with an intact subscapularis tendon. If the patient is unable to lift the hand, then a tear of the subscapularis tendon is suspected.
Lift-off lag test
The examiner will hold the patient’s hand away from the back at the lumbar region and let go. The patient will be unable to keep the hand away from the back if the tendon is torn.
Belly press test
•The patient presses the palm of the hand against the abdomen with the wrist in a neutral position. This is an example of intact subscapularis muscle.
•A positive sign for the belly-press test occurs if the patient is unable to press his belly without wrist volar flexion or the elbow falling posteriorly.
•The shoulder is placed in flexion and maximum internal rotation.
•The examiner positions the patient’s hand on the belly while holding on the flexed elbow.
•If the tendon is ruptured, the patient will not be able to maintain his positions and the hand will lift off of the abdomen when the examiner lets go.
Treatment
Complete tear:
Surgical repair
•Repair may be either open or arthroscopic
•Biceps tenodesis during repair is associated with improved outcomes.
•Biceps tenodesis is usually done if the biceps is involved in the process, otherwise subluxation of the biceps will stress and fail the repair.
Chronic muscle tear
•Pectoral major muscle transfer is the procedure of choice.
The subscapularis muscle is supplied by the upper and lower subscapular nerves. The upper and lower subscapular nerves originate from the posterior cord of the brachial plexus.
The subscapular artery , which is the largest branch of the axillary artery, supplies the subscapularis muscle.
Become a friend on facebook:
Follow me on twitter:
The subscapularis muscles is the largest of the four rotator cuff muscles and it provides about 50% of the total cuff strength.
The subscapularis muscles insert into the lesser tuberosity of the humerus, while the other rotator cuff muscles have an insertion into the greater tuberosity.
The subscapularis muscle acts as a dynamic stabilizer of the humeral head and aids in lifting across the chest. The function of the subscapularis muscle is to adduct and rotate the arm medially.
Posterior dislocation of the humeral head with a “reverse Hills-Sachs lesion” is a rare condition. the condition can be repaired after reduction of the dislocation with the McLaughlin procedure utilizing the subscapularis tendon if the lesion is between 20-40 of the humeral head. The subscapularis tendon is used to fill the reverse Hill-Sachs lesion using suture anchors or screws inserted in the humeral head defect. The screws are inserted into a portion of the lesser tuberosity that is attached to the subscapularis.
At the insertion of the subscapularis tendon into the humerus lies the transverse humeral ligament. the long head of the biceps tendon lies within the bicipital groove and is held in place by the transverse humeral ligament. when a complete rupture of the subscapularis tendon occurs, the transverse humeral ligament may also become torn causing medial dislocation of the biceps tendon from the bicipital groove.
Radiological examination
•Tears of the subscapularis tendon may be diagnosed by using MRI or ultrasound.
•With ultrasound imaging, the probe is placed transversely over the bicipital groove to identify the groove and the biceps tendon while the arm is in a neutral position. The arm is then externally rotated to view the subscapularis tendon.
Diagnosis of the subscapularis rupture
Tears are not common and can be occult. Can be either chronic or acute.
Patient will have
•Pain
•Anterior shoulder swelling
•Decreased range of motion
•The weakness of internal rotation.
Lift-off test
The patient places the hand behind their back at the lumbar level and lifts the hand away form the back with an intact subscapularis tendon. If the patient is unable to lift the hand, then a tear of the subscapularis tendon is suspected.
Lift-off lag test
The examiner will hold the patient’s hand away from the back at the lumbar region and let go. The patient will be unable to keep the hand away from the back if the tendon is torn.
Belly press test
•The patient presses the palm of the hand against the abdomen with the wrist in a neutral position. This is an example of intact subscapularis muscle.
•A positive sign for the belly-press test occurs if the patient is unable to press his belly without wrist volar flexion or the elbow falling posteriorly.
•The shoulder is placed in flexion and maximum internal rotation.
•The examiner positions the patient’s hand on the belly while holding on the flexed elbow.
•If the tendon is ruptured, the patient will not be able to maintain his positions and the hand will lift off of the abdomen when the examiner lets go.
Treatment
Complete tear:
Surgical repair
•Repair may be either open or arthroscopic
•Biceps tenodesis during repair is associated with improved outcomes.
•Biceps tenodesis is usually done if the biceps is involved in the process, otherwise subluxation of the biceps will stress and fail the repair.
Chronic muscle tear
•Pectoral major muscle transfer is the procedure of choice.
The subscapularis muscle is supplied by the upper and lower subscapular nerves. The upper and lower subscapular nerves originate from the posterior cord of the brachial plexus.
The subscapular artery , which is the largest branch of the axillary artery, supplies the subscapularis muscle.
Become a friend on facebook:
Follow me on twitter:
 0:03:15
0:03:15
Subscapularis | Muscle Anatomy
 0:02:01
0:02:01
Subscapularis Muscle - Origin, Insertion, Innervation & Action - Human Anatomy | Kenhub
 0:06:40
0:06:40
Anatomy Of The Subscapularis Muscle - Everything You Need To Know - Dr. Nabil Ebraheim
 0:06:47
0:06:47
Anatomy Of The Subscapularis Muscle - Everything You Need To Know - Dr. Nabil Ebraheim
 0:00:44
0:00:44
The Subscapularis Muscle
 0:00:14
0:00:14
Subscapularis Muscle #physicaltherapy #anatomy_physiology #anatomy #movement #short
 0:06:27
0:06:27
Anatomy of the Subscapularis Muscle
 0:02:39
0:02:39
Subscapularis Anatomy: Origin, Insertion & Action
 0:13:39
0:13:39
Scapula | Bones Of Upper Limb | Anatomy | Sowkya Med Vision
 0:00:18
0:00:18
Subscapularis and teres major
 0:00:57
0:00:57
Subscapularis Muscle : functional anatomy
 0:00:25
0:00:25
Rotator Cuff Tear
 0:03:08
0:03:08
Supraspinatus | Muscle Anatomy
 0:00:30
0:00:30
The Anterior-Posterior Rotator Cuff Force Couple
 0:00:32
0:00:32
Muscles of the shoulder in 30 seconds! #mbbs #medicine #medical #anatomy
 0:04:36
0:04:36
Rotator Cuff Anatomy (Muscles, Actions & Insertions Made Easy)
 0:02:49
0:02:49
Subscapularis: Shoulder Series, Part 9 (3D Animation)
 0:00:45
0:00:45
Understanding the Subscapularis Muscle: Anatomy & Function
 0:00:24
0:00:24
Supraspinatus Anatomy #physicaltherapy #physiotheraphy #anatomy #rotatorcuff
 0:01:08
0:01:08
Rotator Cuff Tear Repair
 0:01:29
0:01:29
Scapular Force Couple - Muscle collaboration in the shoulder
 0:01:39
0:01:39
Subscapularis SpeedFix™ Technique
 0:02:03
0:02:03
Rotator Cuff Injuries | Complete Anatomy
 0:04:28
0:04:28
Infraspinatus | Muscle Anatomy
Комментарии