filmov
tv
Patient Must Come First in Value Based Care

Показать описание
Dr. Sachin Jain wrote an outstanding article on Value Based Care in the April 12, 2022 issue of Forbes stating that the Patient Must Come First in Value Based Care.
Dr. Jain is the CEO of the Medicare Advantage Plan SCAN Health in Southern California.
Dr. Jain Outlines the 7 Tenets of Value Based Care:
A) Managing Hospital Bed-Days
B) Requiring Specialist Referrals
C) Narrow Networks
D) Team-Based Care with NPs, PAs, RNs and MAs
E) Low Cost Prescription Formulary
F) Addressing the Social Determinants of Health
G) Prioritizing Revenue and Profit
Here are 3 Suggestions for how Value Based Care can have the Patient Come First:
1) Put Physicians on Salary and have the variable component of their compensation be made public.
2) Have a 3rd Party Ombudsman that any Patient, Doctor, Nurse or other member of the healthcare team can contact at anytime if they feel a patient is not being put first.
3) Require all doctors, nurses, healthcare workers, administrators, insurance employees and government officials involved in Value Based Care to be on a Value Based Care Insurance Plan themselves.
Sources:
AHealthcareZ is 200+ Healthcare Finance Educational Videos.
AHealthcareZ Viewers Include: Employee Benefits Professionals, HR, CFOs, Insurance Brokers, Benefits Consultants, Doctors and Nurses in Leadership Roles, Hospital and Health System Administrators, Health Insurance Carrier and PBM Professionals, Pharma and Med Device Professionals, Academic Professors and Students in Healthcare Administration and Public Health.
90,000+ Views Per Month Across All Platforms.
Visit AHealthcareZ.com to Subscribe to the Healthcare Finance Video Newsletter.
Dr. Jain is the CEO of the Medicare Advantage Plan SCAN Health in Southern California.
Dr. Jain Outlines the 7 Tenets of Value Based Care:
A) Managing Hospital Bed-Days
B) Requiring Specialist Referrals
C) Narrow Networks
D) Team-Based Care with NPs, PAs, RNs and MAs
E) Low Cost Prescription Formulary
F) Addressing the Social Determinants of Health
G) Prioritizing Revenue and Profit
Here are 3 Suggestions for how Value Based Care can have the Patient Come First:
1) Put Physicians on Salary and have the variable component of their compensation be made public.
2) Have a 3rd Party Ombudsman that any Patient, Doctor, Nurse or other member of the healthcare team can contact at anytime if they feel a patient is not being put first.
3) Require all doctors, nurses, healthcare workers, administrators, insurance employees and government officials involved in Value Based Care to be on a Value Based Care Insurance Plan themselves.
Sources:
AHealthcareZ is 200+ Healthcare Finance Educational Videos.
AHealthcareZ Viewers Include: Employee Benefits Professionals, HR, CFOs, Insurance Brokers, Benefits Consultants, Doctors and Nurses in Leadership Roles, Hospital and Health System Administrators, Health Insurance Carrier and PBM Professionals, Pharma and Med Device Professionals, Academic Professors and Students in Healthcare Administration and Public Health.
90,000+ Views Per Month Across All Platforms.
Visit AHealthcareZ.com to Subscribe to the Healthcare Finance Video Newsletter.
 0:10:55
0:10:55
Patient Must Come First in Value Based Care
 0:00:21
0:00:21
When the Patient Says, “You Too!” Bad Things Happen! #shorts #surgeonlife
 0:00:29
0:00:29
Medical student when their first patient dies #doctors
 0:02:24
0:02:24
Think patient first in everything you do
 0:00:55
0:00:55
The Emergency Physician Admits a Patient
 0:00:21
0:00:21
Day in the life of a psyc ward patient
 0:00:58
0:00:58
My First Day as a DOCTOR
 0:00:22
0:00:22
Falling Patient
 0:00:58
0:00:58
Autism Doctor Meets Autistic Patient……🧑🔬
 0:00:58
0:00:58
General Medicine Treating a Pregnant Patient
 0:05:02
0:05:02
Proper Patient Care - Communication Techniques
 0:01:00
0:01:00
Trying to Discharge a Patient
 0:03:40
0:03:40
Realistic Job Preview : Patient Care Assistant
 0:04:24
0:04:24
Empathy: The Human Connection to Patient Care
 0:00:08
0:00:08
# I C U patient #♥️♥️♥️
 0:01:58
0:01:58
The Role of the Patient Advocate
 0:02:25
0:02:25
Why Are Some Doctors Lacking Empathy? Patient Care Should Come First!
 0:00:59
0:00:59
How to greet a patient?
 0:01:50
0:01:50
Patient Admission: Asking for patient details in English
 0:12:57
0:12:57
Improving Doctor-Patient Communication | Lizzie Cremer | TEDxTrumanStateUniversity
 0:04:11
0:04:11
Cancer Patient Refuses Chemotherapy | Good Morning Britain
 0:19:06
0:19:06
A Day in My Life as a Psych Ward Hospital Patient | VLOG
 0:00:07
0:00:07
Performing Your First Head-To-Toe Assessment On A Real Patient #shorts #nursingschool #nclex
 0:00:15
0:00:15
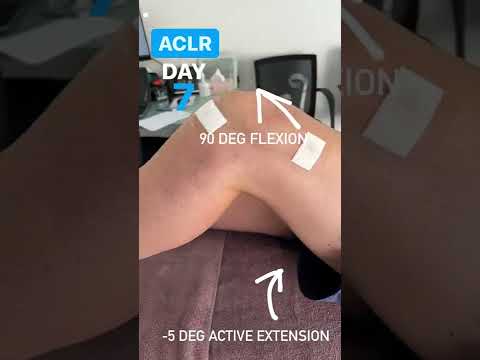
New ACL surgery patient in this week. Here is his active ROM at day 7 post-op.
Комментарии