filmov
tv
Acalculous Cholecystitis

Показать описание
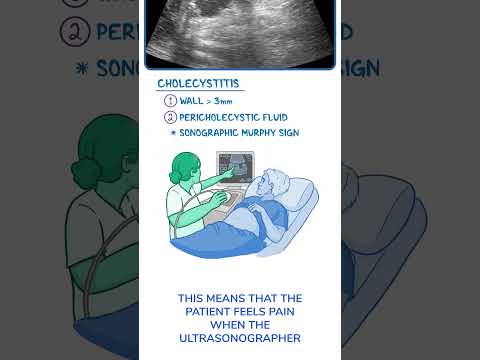
Hello, Acalculous cholecystitis is a gallbladder inflammation without gallstones. Patients can have signs of fever, jaundice, right upper quadrant mass and pain, and Murphy’s sign, which is gallbladder pain induced by your hand when you palpate the gallbladder at the same time as the patient inhale. Patients are usually very ill due to complications of gallbladder inflammation, like Gallbladder necrosis, gangrene, and perforation, that can lead to peritonitis, sepsis, and shock.The lab values can show increased amount of Alkaline phosphatase, Aminotransferases, Bilirubin and Leukocytes. The most important test to make is Ultrasonography. Ultrasonography can show that there are no gallstones or sludge; more than 3 mm gallbladder wall thickening, more than 5 cm gallbladder distension, a striated gallbladder, mucosal sloughing, a positive Murphy’s sign induced by the ultrasonography probe, pericholecystic fluid that indicates perforation that can lead to abscess formation, and “Champagne sign” with gas bubbles in gallbladder fundus. If Ultrasonography is not enough for diagnosis, then Cholescintigraphy, a so-called HIDA scan can be used. But it takes hours to perform, so it’s not recommended in critically ill patients in whom a delay in therapy could be deadly. Here we inject Technetium labeled Hepatic IminoDiacetic Acid that is taken up by liver cells and excreted into bile to the gallbladder. If this does not happen, then it's an indication of acalculous cholecystitis. We can inject Morphine that helps the liver cells to secrete bile into the gallbladder, and thereby makes the diagnosis easier. We treat acalculous cholecystitis with antibiotics and surgery. Before giving antibiotics, we need to take a blood culture. While we wait for the blood culture results, we start a broad-spectrum antibiotic combination, like Ampicillin-Sulbactam, or Piperacillin-Tazobactam, or Ticarcillin-Clavulanate, or Ceftriaxone-Metronidazole. When we get the blood culture results we start to treat the specific microbes that infect the gallbladder, like for example Bacteroides, Escherichia coli, Enterococcus faecalis, Klebsiella, Methicillin-resistant Staphylococcus aureus (MRSA), Pseudomonas, or Proteus species. Then it’s very important to surgically operate as soon as possible. We usually start with a Cholecystostomy. But if we don’t see an improvement within 24 hours after the operation, we start Cholecystectomy immediately. Sometimes, when there is gallbladder necrosis, perforation, or emphysematous cholecystitis, we start with Cholecystectomy right from the beginning. Thank you very much for listening!
 0:02:43
0:02:43
Acalculous Cholecystitis
 0:04:28
0:04:28
Acalculous Gallbladder Disease
 0:07:26
0:07:26
Identifying acute cholecystitis
 0:01:09
0:01:09
Acalculous Cholecystitis Findings
 0:12:38
0:12:38
Acute Cholecystitis - Overview (signs and symptoms, pathophysiology, treatment)
 0:00:44
0:00:44
acalculous cholecystitis
 0:03:53
0:03:53
WHAT IS ACUTE ACALCULOUS CHOLECYSTITIS?
 0:00:58
0:00:58
Diagnostics on Demand: Cholecystitis
 0:00:32
0:00:32
Acute acalculous cholecystitis
 0:07:49
0:07:49
Understanding Acute Cholecystitis
 0:13:45
0:13:45
ACALCULOUS CHOLECYSTITIS - Quick Review - By Pramil Cheriyath MD
 0:00:28
0:00:28
acalculous cholecystitis
 0:06:14
0:06:14
Acute Cholecystitis (Gallbladder Attack) Made Simple
 0:00:36
0:00:36
Treatment Of Acute Cholecystitis : Quick Bites Internal medicine (Gastroenterology)
 0:44:41
0:44:41
A Class On Acalculous cholecystitis By Dr Raviteja Dept Of General Surgery
 0:00:52
0:00:52
Acalculous cholecystitis
 0:17:57
0:17:57
Acute Cholecystitis
 0:01:48
0:01:48
Management of Acute cholecystitis | Gallbladder inflammation with Gall Stone - Dr. Nanda Rajaneesh
 0:05:06
0:05:06
A Calculous Cholecystitis Symptoms and Causes | Explained By Gastroenterologist Dr.V Sunil Kumar
 0:03:34
0:03:34
Acalculous cholecystitis #neetpg #fmge #usmle
 0:02:54
0:02:54
Acalculus Cholecystitis #cholecystitis #GBwalledema #acalculuscholecystitis
 0:01:53
0:01:53
Is it possible to have gallbladder symptoms without gallstones?
 0:00:09
0:00:09
Acalculous cholecystitis treatment - unstable patient
 0:01:00
0:01:00
#icushort 291: Very serious complication of long term TPN- acalculous cholecystitis #esbicm
Комментарии