filmov
tv
Intensity of First Sound s1 | Heart Sounds | cardiology

Показать описание
The intensity of S1 depends upon: the position of the AV valves at the onset of ventricular systole, the structure of the leaflets themselves, and the rate of pressure rise in the ventricle. Normally, S1 is louder than S2 at the apex, and softer than S2 at the base of the heart. Pathologic changes in the intensity of S1 relative to S2 may be seen in certain disease states. When evaluating the intensity of S2, note the relative intensity of the aortic component (A2) and the pulmonic component (P2). Normally A2 is louder than P2.
The first heart sound is made up of several components, although the most audible components heard at the bedside are the high frequency vibrations related to mitral and tricuspid closure. Generally, the louder sound of mitral closure drowns out the softer sound of tricuspid closure. Occasionally the two are separated sufficiently such that there is audible splitting of S1, heard best at the apex or lower left sternal border. Like S1, S2 is made up of several components. The most audible are the high frequency components attributable to the closure of the aortic and pulmonic valves.
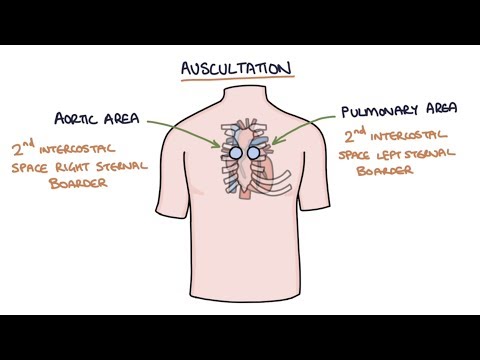
When evaluating for splitting, listen in the 2nd and 3rd left intercostal spaces. Ask the patient to breathe quietly, and then a bit more deeply. During inspiration you should hear the inspiratory splitting of S2 into A2 and P2. To the untrained ear this sounds more like a prolongation of sound rather than two distinct sounds. In general the interval between A2 and P2 is quite short, although in some situations the patient may have a widened interval. Next, listen for splitting of S2 to disappear during expiration. If there is splitting during expiration, this is abnormal and is termed paradoxical splitting.
#sound #health #medical
The first heart sound is made up of several components, although the most audible components heard at the bedside are the high frequency vibrations related to mitral and tricuspid closure. Generally, the louder sound of mitral closure drowns out the softer sound of tricuspid closure. Occasionally the two are separated sufficiently such that there is audible splitting of S1, heard best at the apex or lower left sternal border. Like S1, S2 is made up of several components. The most audible are the high frequency components attributable to the closure of the aortic and pulmonic valves.
When evaluating for splitting, listen in the 2nd and 3rd left intercostal spaces. Ask the patient to breathe quietly, and then a bit more deeply. During inspiration you should hear the inspiratory splitting of S2 into A2 and P2. To the untrained ear this sounds more like a prolongation of sound rather than two distinct sounds. In general the interval between A2 and P2 is quite short, although in some situations the patient may have a widened interval. Next, listen for splitting of S2 to disappear during expiration. If there is splitting during expiration, this is abnormal and is termed paradoxical splitting.
#sound #health #medical
 0:01:36
0:01:36
 0:02:54
0:02:54
 0:25:53
0:25:53
 0:02:04
0:02:04
 0:02:07
0:02:07
 0:19:00
0:19:00
 0:11:10
0:11:10
 0:01:29
0:01:29
 0:16:15
0:16:15
 0:00:20
0:00:20
 0:07:48
0:07:48
 0:19:10
0:19:10
 0:31:28
0:31:28
 0:08:04
0:08:04
 0:01:53
0:01:53
 0:02:29
0:02:29
 0:02:53
0:02:53
 0:12:07
0:12:07
 0:09:02
0:09:02
 1:01:01
1:01:01
 0:00:12
0:00:12
 0:00:26
0:00:26
 0:01:45
0:01:45
 0:00:41
0:00:41