filmov
tv
Hypernatremia

Показать описание
A review of hypernatremia, including physiology, etiologies, diagnostic work-up, and treatment. Particular focus given to diabetes insipidus.
 0:25:55
0:25:55
Hypernatremia
 0:13:52
0:13:52
Hypernatremia Explained! Types, Diagnosis, & Treatment
 0:14:05
0:14:05
Hypernatremia - Examples
 1:14:34
1:14:34
Hypernatremia
 0:15:55
0:15:55
Hypernatremia Explained Clearly - Pathophysiology & Treatment
 0:34:27
0:34:27
Hypernatremia approach and management-MD/DCH/DNB pediatrics exam preparation
 0:08:57
0:08:57
Hypernatremia
 0:11:16
0:11:16
Hypernatremia in Nursing
 0:02:10
0:02:10
Electrolyte Imbalances | Hyponatremia (Low Sodium)
 0:03:11
0:03:11
Hypernatremia Overview (Part 1) | Sketchy Medical | USMLE Step 2 CK
 0:23:02
0:23:02
HYPERNATREMIA | Causes | Clinical Features | Diagnosis | Treatment | Harrison
 0:26:30
0:26:30
Hypernatremia | Pathophysiology, Etiologies, Consequences, and Treatment
 0:16:34
0:16:34
Hypernatremia
 0:25:55
0:25:55
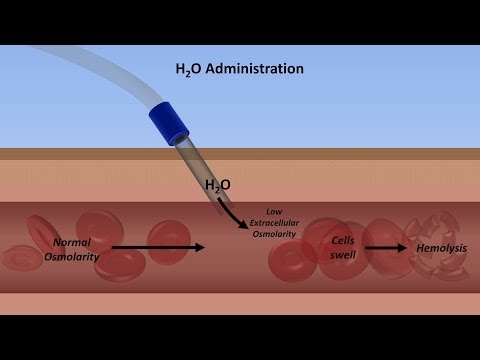
Sodium and Water - Electrolytes - Osmosis - Osmotic Pressure - Fluids and Electrolytes Series
 0:34:53
0:34:53
Disorders of Sodium: Hypo- and Hypernatremia with Alexandra Reynolds, MD
 0:11:30
0:11:30
Hypernatremia Made Easy
 0:01:44
0:01:44
Hypernatremia | Causes, Symptoms & Diagnosis Of Hypernatremia | Sodium Normal Ranges |
 0:29:06
0:29:06
Hypernatremia for USMLE Step 2
 0:11:08
0:11:08
HYPONATREMIA/HYPERNATREMIA Med Surg Nursing
 3:09:54
3:09:54
Hyponatremia
 0:01:32
0:01:32
Check out that Salt MODEL! Causes of Hypernatremia... Nursing Mnemonics
 0:03:56
0:03:56
Hypernatremia | Medicine Video Lectures | Medical Student | V-Learning | sqadia.com
 0:16:20
0:16:20
Hypernatremia When, why and how?
 0:15:24
0:15:24
Hyponatremia
Комментарии