filmov
tv
Understanding Diffuse Large B-Cell Lymphoma with Bruce Cheson, MD, FACP, FAAAS, FASCO

Показать описание
Bruce Cheson, MD, FACP, FAAAS, FASCO gives a deep dive into Diffuse Large B-Cell Lymphoma.
About Dr. Cheson: Bruce Cheson, MD, FACP, FAAAS, FASCO, Georgetown University Hospital | Lombardi Comprehensive Cancer Center.
The Lymphoma Research Foundation is the nation's largest non-profit organization devoted to funding innovative research and providing people with lymphoma and healthcare professionals with up-to-date information about this type of cancer.
LEARN MORE!
About Dr. Cheson: Bruce Cheson, MD, FACP, FAAAS, FASCO, Georgetown University Hospital | Lombardi Comprehensive Cancer Center.
The Lymphoma Research Foundation is the nation's largest non-profit organization devoted to funding innovative research and providing people with lymphoma and healthcare professionals with up-to-date information about this type of cancer.
LEARN MORE!
 0:10:09
0:10:09
Understanding Diffuse Large B-Cell Lymphoma with Jennifer Amengual, MD
 0:04:54
0:04:54
Understanding Diffuse Large B-Cell Lymphoma (DLBCL)
 0:09:16
0:09:16
Understanding Diffuse Large B-Cell Lymphoma
 0:10:07
0:10:07
Understanding Diffuse Large B-Cell Lymphoma with Bruce Cheson, MD, FACP, FAAAS, FASCO
 0:12:18
0:12:18
Understanding Diffuse Large B-Cell Lymphoma
 0:05:37
0:05:37
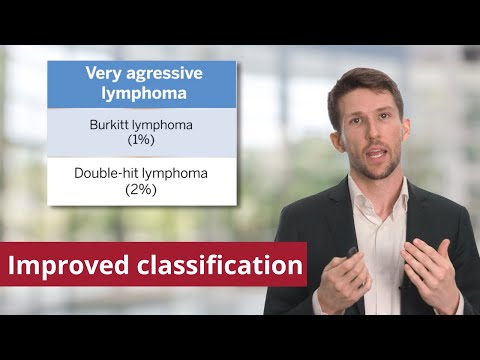
Understanding Diffuse Large B-cell Lymphoma (DLBCL) and Its Subtypes
 0:08:21
0:08:21
Diffuse Large B-Cell Lymphoma (DLBCL) - Aggressive B-Cell Neoplasm - Non-Hodgkin’s Lymphoma
 0:03:20
0:03:20
Diffuse Large B-Cell Lymphoma for Newly Diagnosed Patients
 0:03:36
0:03:36
How Is Diffuse Large B-Cell Lymphoma Explained to a Newly Diagnosed Patient?
 0:00:19
0:00:19
What is diffuse large B-cell lymphoma?
 0:01:46
0:01:46
Diffuse large B-cell lymphoma diagnosis and treatment
 0:04:47
0:04:47
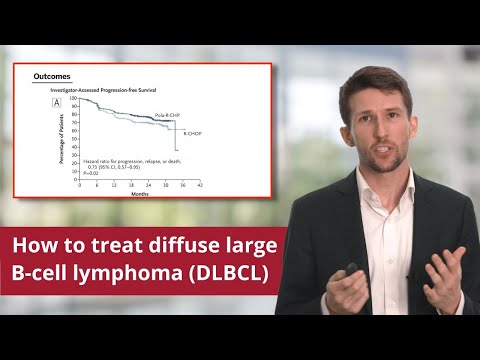
The Polarix Trial: Initial Therapy of Diffuse Large B-cell Lymphoma
 0:06:41
0:06:41
Diffuse Large B-cell Lymphoma (DLBCL): Understanding the Treatment Landscape
 0:12:21
0:12:21
Non-hodgkin lymphoma - causes, symptoms, diagnosis, treatment, pathology
 0:07:24
0:07:24
Lymphoma: Overview of Classification
 0:03:48
0:03:48
What Do You Need to Know about Diffuse Large B-Cell Lymphoma (DLBCL)?
 0:46:48
0:46:48
Relapsed and Refractory Diffuse Large B-Cell Lymphoma
 0:12:46
0:12:46
Understanding CAR T-cell Therapy in Lymphoma
 0:04:26
0:04:26
Non-Hodgkin Lymphoma: Symptoms & Treatment | Stanford
 0:06:14
0:06:14
An Expert Defines Diffuse Large B-Cell Lymphoma (DLBCL)
 0:03:04
0:03:04
Future directions for the treatment of diffuse large B-cell lymphoma
 0:03:00
0:03:00
What Is Diffuse Large B-cell Lymphoma (DLBCL)?
 0:01:49
0:01:49
How Do Different Diffuse Large B-Cell Lymphoma Subtypes Impact Treatment Options?
 0:03:10
0:03:10
Clinical Trials and Research for Diffuse Large B-Cell Lymphoma
Комментарии