filmov
tv
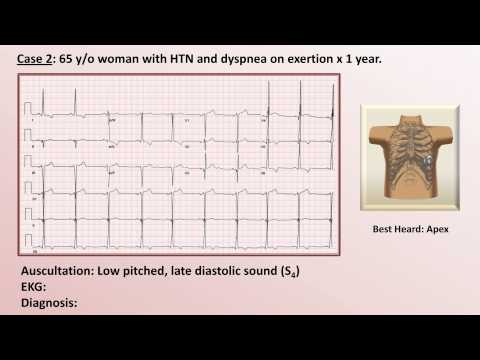
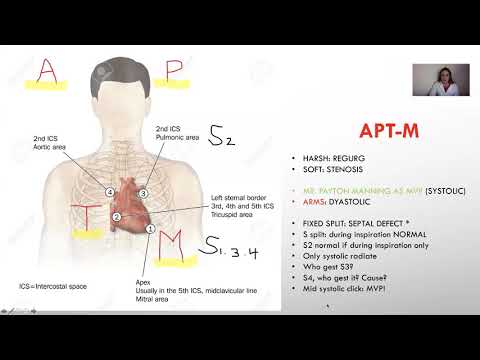
EKG and Heart Murmur Review - Part 1

Показать описание
A review of basic EKG interpretation and cardiac auscultation, using actual clinical cases to demonstrate connections between patient symptoms, EKG findings, and abnormalities of auscultation. I recommend first viewing my videos on "Heart Murmurs", "Heart Sounds", "Intro to EKG: Rate and Axis", and "Intro to EKG: Chamber Enlargement", as this review will rely heavily on information present during those lectures.
I highly recommend watching in 1080p.
I highly recommend watching in 1080p.
EKG and Heart Murmur Review - Part 1

EKG and Heart Murmur Review - Part 2

EKG like a BOSS Part 1 - How to Read EKGs (ECG interpretation for nurses)

Learn Heart Murmurs In 10 Minutes (With Heart Murmur Sounds)

Heart Sounds 🔈🫀

Heart Murmurs Review | | Mnemonics And Proven Ways To Memorize for your exams!

Heart Sounds & Murmurs | Clinical Medicine
Heart Murmurs | Locations, Maneuvers, Buzzwords

NP Learning: Cardiac Murmurs

Heart sounds in different conditions #volumeup

Heart Sound Locations & Murmurs for Nursing | Cardiac Assessment
MURMURS for NP boards [OLD VERSION], improved one👇

Save this trick to never forget valves & murmurs again!🫀#medschool #medstudent #cardiology #usml...

Ace Heart Murmurs | Mnemonics for NP Boards exams

Most Common ECG Patterns You Should Know
Heart Sounds | S1 S2 S3 S4 and Murmurs Nursing Assessment

Heart Murmur ECG EKG Electrocardiogram Uri Ben-Zur MD

Cardiology Review, for NP boards

What to expect for an echocardiogram

ECG Red Flags for Syncope and Pre-Syncope

Hypertrophic Cardiomyopathy Made Simple

ECG Interpretation | Clinical Medicine

Echocardiogram NORMAL vs ABNORMAL! #radiology #cardiology

Lub Dub (S1 & S2) Heart Sounds Anatomy Explained in 30 Seconds #shorts
Комментарии