filmov
tv
Inpatient Diabetes Management
Показать описание
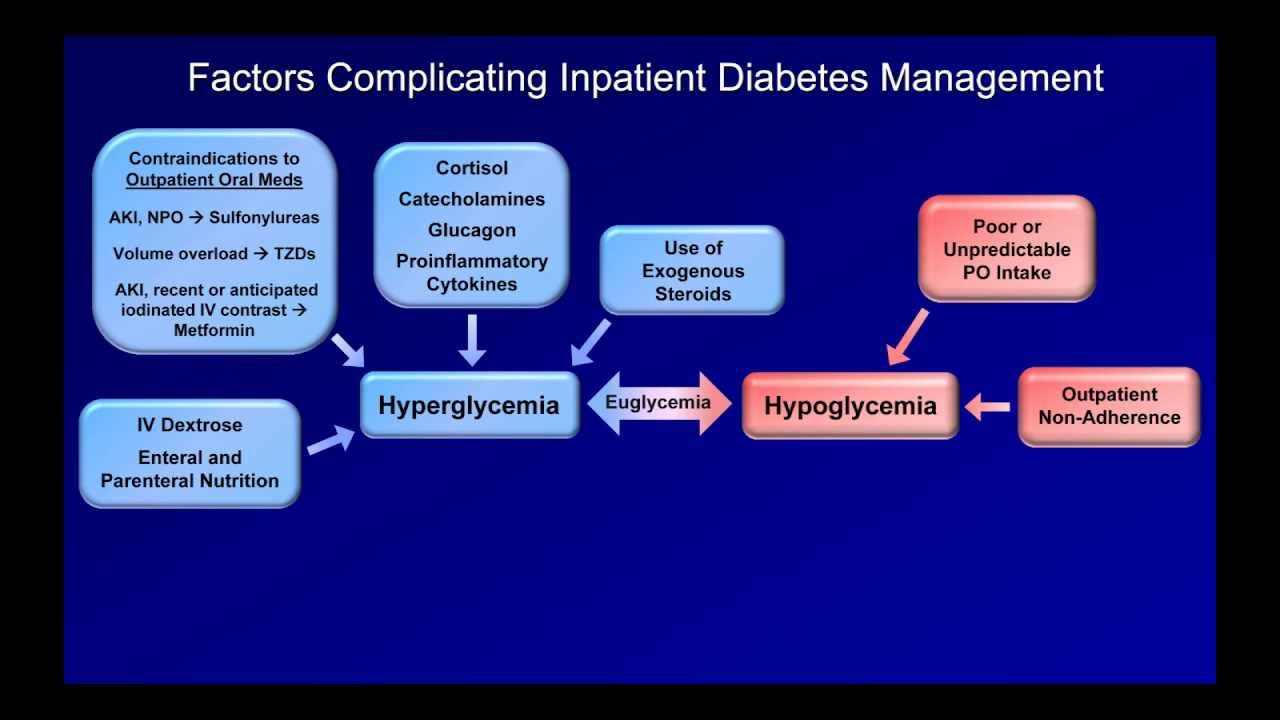
A summary of the inpatient management of diabetes. Topics include the sliding scale, basal bolus regimens, adjusting insulin when NPO, adjusting insulin for persistent hyperglycemia, and the consistent carb diet.
Information here is provided for educational purposes only, and is not intended to substitute for the opinion of an experienced and licensed health care professional.
Information here is provided for educational purposes only, and is not intended to substitute for the opinion of an experienced and licensed health care professional.
 0:22:54
0:22:54
Inpatient Diabetes Management
 0:58:31
0:58:31
Management of Inpatient Diabetes and Hyperglycemia
 0:09:49
0:09:49
Inpatient Diabetes Management
 0:18:14
0:18:14
Inpatient Management of Diabetes
 0:06:45
0:06:45
How to Order an Insulin Regimen
 0:50:40
0:50:40
Inpatient Glucose Management by Dr. Sathya Krishnasamy
 1:02:26
1:02:26
Management of Diabetes in 2023: Updates and Future Directions
 0:12:38
0:12:38
INSULIN TREATMENT FOR DIABETES | HOW TO START INSULIN ON A PATIENT | DIABETES MELLITUS TREATMENT |
 0:53:35
0:53:35
The Environmental Impact of Short Stay Total Shoulder Arthroplasty
 1:01:47
1:01:47
August 11, 2021 Inpatient Diabetes Management, Rebecca Leary, DO
 0:11:57
0:11:57
Inpatient Diabetes Management. Why Sliding Scale is WRONG, and Basal Bolus is Better.
 0:59:11
0:59:11
INPATIENT MANAGEMENT OF HYPERGLYCEMIA
 0:37:00
0:37:00
Inpatient management of diabetes 1
 0:10:48
0:10:48
Glucose Monitoring in the Hospital: Best Practices for Inpatient Diabetes Management
 0:18:57
0:18:57
IM: Inpatient insulin management
 1:19:18
1:19:18
The Curbsiders Internal Medicine Podcast - #330 Inpatient Diabetes with Dr. Dave Lieb (Part 1)
 0:03:03
0:03:03
Inpatient Diabetes Management | UPMC
 0:13:13
0:13:13
25 Inpatient Diabetes Management
 0:55:30
0:55:30
2021 Dr. Mary Ann Emanuele - Inpatient Diabetes Management
 0:03:01
0:03:01
Inpatient Diabetes Management by Elizabeth D. Nelson, APRN, CNP | Preview
 0:20:01
0:20:01
Dr. Guillermo Umpierrez: Managing In-Hospital Hyperglycemia
 0:57:25
0:57:25
The American Diabetes Association’s Standards of Care in Diabetes—2024
 0:54:12
0:54:12
'Updates in Management of Hyperglycemia in Hospitalized Patients' by Laleh Razavi, MD
 0:14:52
0:14:52
Inpatient Insulin Sliding Scales Explained! What is Sliding Scale Insulin Diabetes
Комментарии