filmov
tv
Femoral Neck Fractures Fixation - Everything You Need To Know - Dr. Nabil Ebraheim
Показать описание
Dr. Ebraheim’s educational animated video describes femoral neck fracture fixation.
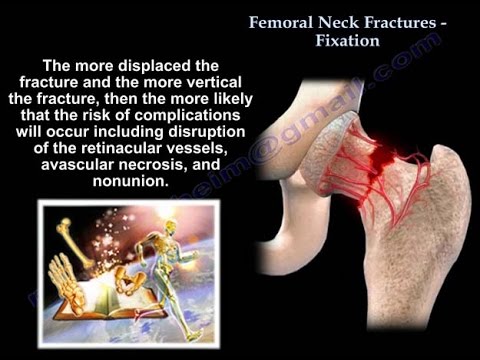
Anatomy : The neck shift angle is approximately 130°. Anteversion is approximately 10°. No periosteum in the femoral neck and no abundant callus. The fracture heals by endosteal proliferation. The medial femoral circumflex is the most important blood supply to the femoral head (lateral epiphyseal artery). In young patients, injury is usually high energy that may lead to avascular necrosis. Some believe that surgery should be urgent in the young patient in order to decompress the compressed vessels. The more displaced the fracture and the more vertical the fracture, then the more likely that the risk of complications will occur including disruption of the retinacular vessels, avascular necrosis and nonunion. Femoral neck reduction should be anatomic, either by closed technique or open technique (if closed reduction technique fails).The calcar is an area of stress transfer. It is a posteomedial dense plate of bone. It forms an internal strut within the inferior portion of the femoral neck and intertrochanteric area.
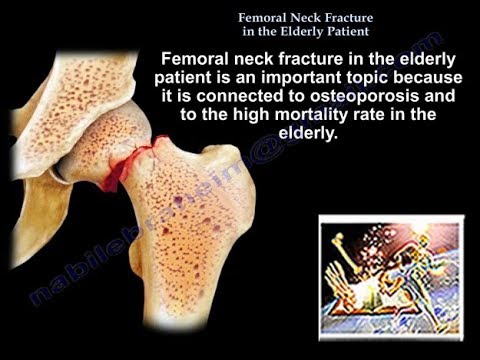
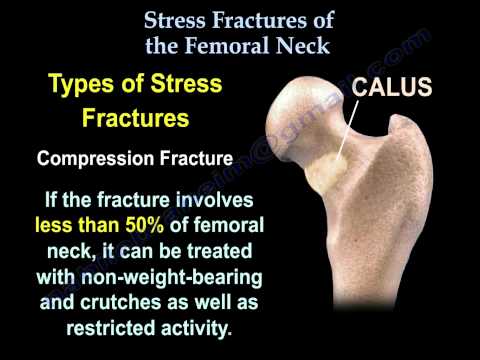
Mechanism of Injury: Low energy fracture occurs in the elderly from a fall onto the greater trochanter. A fall in the elderly is different than a fall in the young. The older patient has less protective reflexes during a fall. The younger patient has better protective reflexes during a fall. Wrist fractures occur in the younger group than fractures of the hip. The young will try to protect themselves by falling on the wrist. High energy fractures can occur in the young or the elderly from either a fall or a car accident. Stress fractures can occur in athletes. Insufficiency fracture in the elderly (occult).
History: Obtain adequate history from the patient such as any syncopal episodes and loss of consciousness. The preinjury ambulatory status may determine the treatment selected for the patient. Falls and low sodium will increase the risk of hip fractures.
Clinical Exam: Position of leg is usually shortening and external rotation.
Patient Mortality: 1 year mortality rate is approximately 30%. Surgery delay more than 4 days may double the mortality rates (these patients are probably sicker than the average patient). Medical comorbidities (4 or more increases mortality). Renal patients with hip fractures are a problem. Institutionalized patients and low sodium levels may also be risk factors.
Surgical Timing: The optimal time for surgery is after medical stabilization. There is an improved outcome if surgery is done within 48 hours. Surgical delay up to 72 hours for medicals stabilization is warranted in unhealthy patients.
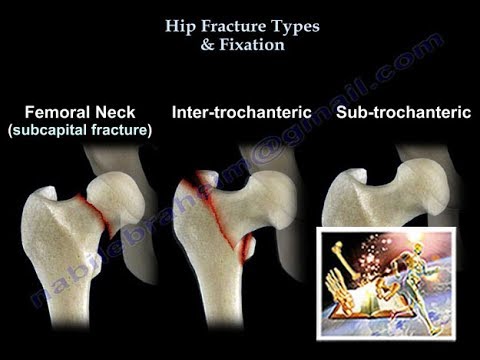
Surgery: Displacement and physiological age of the patient will decide the treatment. Nondisplaced fractures should be fixed to prevent displacement. This is done for the young and older patients and it is a minimal surgery. Screws are placed in an inverted triangular pattern with inferior screws posterior to the midline and adjacent to the calcar. If the fracture is displaced and the patient is young, you will do closed reduction or open reduction to have the fracture be anatomic (reduction of the fracture should be anatomic). Avoid malreduction! Adequacy of reduction is the most important factor. A healed femoral neck fracture with shortening is associated with a poor functional outcome.
Treatment: Treatment for a displaced fracture in active elderly patients will be a total hip replacement. It is also used in patients with degenerative arthritis or rheumatoid arthritis and femoral neck fractures. Treatment for a displaced fracture in debilitated, inactive elderly patients will be a bipolar or unipolar hip replacement.
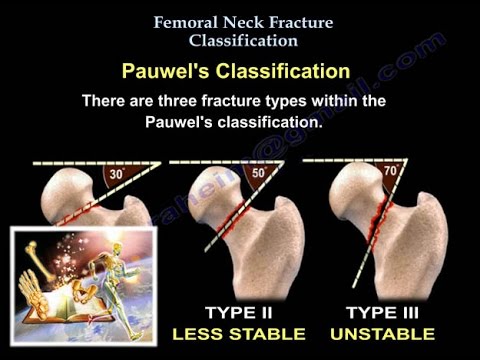
Surgery for Nonunion: Valgus Intertrochanteric Osteotomy in the young will change the orientation of the fracture from vertical (biomechanically bad) to horizontal (biomechanically good).
Follow me on twitter:
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
Anatomy : The neck shift angle is approximately 130°. Anteversion is approximately 10°. No periosteum in the femoral neck and no abundant callus. The fracture heals by endosteal proliferation. The medial femoral circumflex is the most important blood supply to the femoral head (lateral epiphyseal artery). In young patients, injury is usually high energy that may lead to avascular necrosis. Some believe that surgery should be urgent in the young patient in order to decompress the compressed vessels. The more displaced the fracture and the more vertical the fracture, then the more likely that the risk of complications will occur including disruption of the retinacular vessels, avascular necrosis and nonunion. Femoral neck reduction should be anatomic, either by closed technique or open technique (if closed reduction technique fails).The calcar is an area of stress transfer. It is a posteomedial dense plate of bone. It forms an internal strut within the inferior portion of the femoral neck and intertrochanteric area.
Mechanism of Injury: Low energy fracture occurs in the elderly from a fall onto the greater trochanter. A fall in the elderly is different than a fall in the young. The older patient has less protective reflexes during a fall. The younger patient has better protective reflexes during a fall. Wrist fractures occur in the younger group than fractures of the hip. The young will try to protect themselves by falling on the wrist. High energy fractures can occur in the young or the elderly from either a fall or a car accident. Stress fractures can occur in athletes. Insufficiency fracture in the elderly (occult).
History: Obtain adequate history from the patient such as any syncopal episodes and loss of consciousness. The preinjury ambulatory status may determine the treatment selected for the patient. Falls and low sodium will increase the risk of hip fractures.
Clinical Exam: Position of leg is usually shortening and external rotation.
Patient Mortality: 1 year mortality rate is approximately 30%. Surgery delay more than 4 days may double the mortality rates (these patients are probably sicker than the average patient). Medical comorbidities (4 or more increases mortality). Renal patients with hip fractures are a problem. Institutionalized patients and low sodium levels may also be risk factors.
Surgical Timing: The optimal time for surgery is after medical stabilization. There is an improved outcome if surgery is done within 48 hours. Surgical delay up to 72 hours for medicals stabilization is warranted in unhealthy patients.
Surgery: Displacement and physiological age of the patient will decide the treatment. Nondisplaced fractures should be fixed to prevent displacement. This is done for the young and older patients and it is a minimal surgery. Screws are placed in an inverted triangular pattern with inferior screws posterior to the midline and adjacent to the calcar. If the fracture is displaced and the patient is young, you will do closed reduction or open reduction to have the fracture be anatomic (reduction of the fracture should be anatomic). Avoid malreduction! Adequacy of reduction is the most important factor. A healed femoral neck fracture with shortening is associated with a poor functional outcome.
Treatment: Treatment for a displaced fracture in active elderly patients will be a total hip replacement. It is also used in patients with degenerative arthritis or rheumatoid arthritis and femoral neck fractures. Treatment for a displaced fracture in debilitated, inactive elderly patients will be a bipolar or unipolar hip replacement.
Surgery for Nonunion: Valgus Intertrochanteric Osteotomy in the young will change the orientation of the fracture from vertical (biomechanically bad) to horizontal (biomechanically good).
Follow me on twitter:
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
 0:10:03
0:10:03
Femoral neck fracture fixation. hip fracture examination , x rays , treatment and surgery
 0:04:17
0:04:17
Femoral Neck - Fracture - Fixation Using the 7.3 mm Cannulated Screw
 0:08:22
0:08:22
Femoral Neck Fracture Classification - Everything You Need To Know - Dr. Nabil Ebraheim
 0:09:22
0:09:22
Neck of Femur Fractures | Expert Physio Review
 0:17:56
0:17:56
Optimal management of the displaced femoral neck fractures in the elderly
 0:09:56
0:09:56
Understanding Neck of Femur Fractures
 0:03:52
0:03:52
Femoral Neck fracture Classifications - Everything You Need To Know - Dr. Nabil Ebraheim
 0:12:48
0:12:48
Understanding Hip Fractures and Hip Surgery
 0:46:07
0:46:07
Orthopaedic Surgery in One Go: Revision
 0:06:09
0:06:09
Femoral Neck Fractures and Exercise
 0:05:29
0:05:29
Femoral Neck Fracture In The Elderly Patient - Everything You Need To Know - Dr. Nabil Ebraheim
 0:08:26
0:08:26
Femoral Neck Fracture Nonunion - Everything You Need To Know - Dr. Nabil Ebraheim
 0:00:52
0:00:52
Femoral Neck Fractures
 0:04:43
0:04:43
Hip Fracture Types & Fixation - Everything You Need To Know - Dr. Nabil Ebraheim
 0:34:09
0:34:09
Controversies in hip and femur fracture management
 1:13:06
1:13:06
AO Trauma NA Orthopaedic Trauma Journal Club Series— Elderly Femoral Neck Fractures
 0:03:37
0:03:37
Ipsilateral Femoral Neck & Shaft Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
 0:14:12
0:14:12
Proximal Femur Fractures Femoral neck fractures 2
 0:00:13
0:00:13
How to Nail a Hip Fracture 🔨 #shorts
 0:03:45
0:03:45
Femoral neck stress fracture: Signs, symptoms, diagnosis, and treatment
 0:12:19
0:12:19
Femoral neck fractures in patients younger than 50 years - 1 of 3
 0:02:53
0:02:53
Treatment of Displaced Femoral Neck Fracture in Patients Aged 55 to 70 Years
 0:10:04
0:10:04
Proximal Femur Fractures Femoral Neck Fractures 1
 0:02:52
0:02:52
Stress Fractures Of The Femoral Neck - Everything You Need To Know - Dr. Nabil Ebraheim
Комментарии